The Glasgow Coma Scale (GCS) is the most widely used neurological assessment tool in intensive care medicine. Developed in 1974, it provides a standardised method for evaluating consciousness by scoring three independent components — eye opening, verbal response, and motor response — yielding a total score from 3 (deep coma) to 15 (fully alert).
In ICU practice, the GCS is not just a clinical tool. It feeds directly into severity scoring systems like SOFA and APACHE II, forms the basis of treatment escalation decisions, and appears as a critical data point in medicolegal records and insurance documentation. An incorrectly recorded or incompletely documented GCS can undermine clinical assessments, skew severity scores, and weaken medicolegal defence.
This guide covers every component of the GCS in detail, explains how to score accurately in common ICU scenarios, introduces the pediatric GCS for younger patients, and addresses the documentation standards required for clinical, insurance, and legal purposes.

What Is the Glasgow Coma Scale?
The Glasgow Coma Scale was developed by Graham Teasdale and Bryan Jennett at the University of Glasgow in 1974. It was originally designed to standardise the assessment of impaired consciousness in head injury patients, but its utility quickly expanded to all forms of acute brain injury, metabolic encephalopathy, post-cardiac arrest care, and general ICU monitoring.
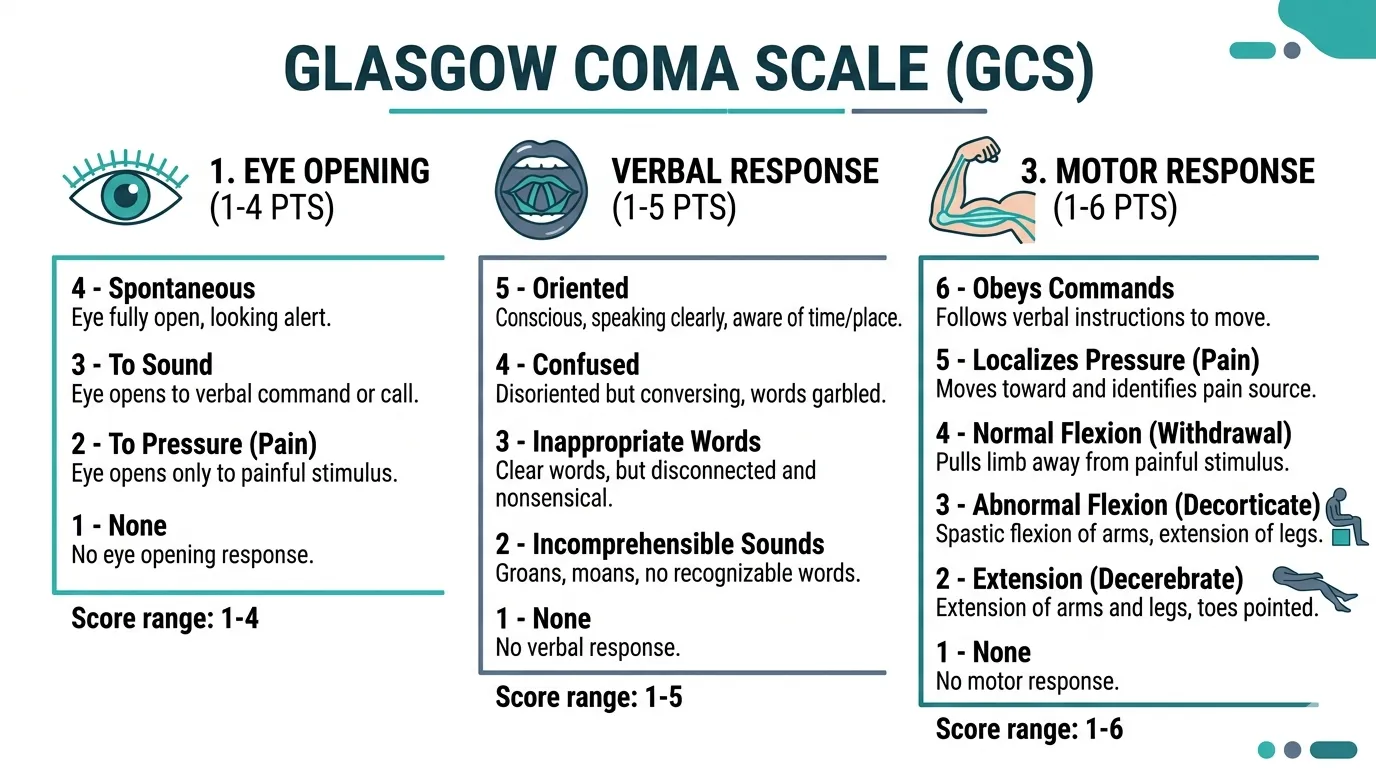
The GCS evaluates three behavioural responses independently:
- Eye Opening (E) — scored 1 to 4
- Verbal Response (V) — scored 1 to 5
- Motor Response (M) — scored 1 to 6
Total GCS = E + V + M, ranging from 3 (no response in any component) to 15 (fully oriented and obeying commands).
The three components are assessed and documented separately because the total score alone can obscure clinically important differences. A GCS of 8 could represent E2V2M4, E4V1M3, or E1V2M5 — each with a very different clinical picture and prognosis.
Always document GCS as the component breakdown (E + V + M = total), not just the total score. A GCS of 7 in a patient with E1V1M5 (localising pain but no eye or verbal response) has a fundamentally different prognosis than E2V2M3 (flexion withdrawal only). The breakdown matters for clinical decision-making, severity scoring, and medicolegal documentation.
GCS Components: Detailed Scoring Guide
Eye Opening (E): Score 1–4
The eye opening component assesses the arousal mechanism of the brainstem reticular activating system.
| Score | Response | How to Assess |
|---|---|---|
| E4 | Spontaneous | Eyes open without stimulation. Patient may or may not be aware. |
| E3 | To speech | Eyes open in response to verbal command or speech (not necessarily to specific instructions). |
| E2 | To pressure | Eyes open only in response to peripheral or central painful stimulus (e.g., trapezius squeeze, nail bed pressure). |
| E1 | None | No eye opening to any stimulus. |
If the patient’s eyes are closed due to swelling (periorbital oedema, facial trauma), record as “NT” (not testable) for the eye component, not E1. Scoring E1 when the eyes are physically unable to open misrepresents the patient’s neurological status and inflates severity scores.
Verbal Response (V): Score 1–5
The verbal component assesses language function and higher cortical integration.
| Score | Response | How to Assess |
|---|---|---|
| V5 | Oriented | Patient knows who they are, where they are, and the date/time. |
| V4 | Confused | Patient speaks in sentences but is disoriented to person, place, or time. |
| V3 | Inappropriate words | Recognisable words but no sustained conversational exchange. Random or exclamatory speech. |
| V2 | Incomprehensible sounds | Moaning, groaning — no recognisable words. |
| V1 | None | No verbalisation to any stimulus. |
In intubated patients, the verbal component cannot be assessed. Record as “VT” (verbal — tube in situ) or “V1T” to indicate the tube is the reason for the absent verbal response. Never assign V1 to an intubated patient without the “T” qualifier — this falsely suggests neurological absence of speech rather than a mechanical inability to speak. Some units report the GCS as “E_M_VT” to make this explicit.
Motor Response (M): Score 1–6
The motor component is the most clinically informative and carries the greatest prognostic weight of the three GCS components.
| Score | Response | How to Assess |
|---|---|---|
| M6 | Obeys commands | Patient performs requested movements (e.g., “lift your arms”, “wiggle your toes”). |
| M5 | Localises pain | Patient reaches toward and attempts to remove the source of a painful stimulus (e.g., reaches across the body to the site of a central stimulus). |
| M4 | Normal flexion (withdrawal) | Patient flexes/withdraws the limb away from painful stimulus but does not localise. |
| M3 | Abnormal flexion | Stereotypical flexion of the arm at the elbow, often with wrist flexion and adduction (decorticate posturing). |
| M2 | Extension | Extension and internal rotation of the arm with wrist pronation (decerebrate posturing). |
| M1 | None | No motor response to any stimulus. |
The distinction between M5 (localising) and M4 (withdrawal) is the most commonly misscored element of the GCS. Localising means the patient’s hand crosses the midline or rises above the clavicle to reach the stimulus source. Withdrawal is a pulling-away movement without purposeful reaching. When in doubt, apply a central stimulus (trapezius squeeze) rather than peripheral (nail bed pressure) to differentiate these responses.
GCS Score Interpretation
Total Score Classification
| GCS Total | Classification | Clinical Significance |
|---|---|---|
| 15 | Normal | Fully conscious and oriented |
| 13–14 | Mild impairment | Alert but may be confused or mildly obtunded |
| 9–12 | Moderate impairment | Significant obtundation, may still localise pain |
| 3–8 | Severe impairment (coma) | Generally requires airway protection and intubation |
A GCS of 8 or below is the traditional threshold for intubation and airway protection, though clinical context always takes precedence. A patient with GCS 9 who is rapidly deteriorating may need intubation sooner, while a patient with a stable GCS of 7 from a chronic metabolic cause may not need immediate intubation if the airway is being maintained.
GCS and the SOFA Score
The GCS is one of the six organ system assessments in the SOFA score, mapping directly to the CNS component:
| GCS | SOFA CNS Score |
|---|---|
| 15 | 0 — normal |
| 13–14 | 1 |
| 10–12 | 2 |
| 6–9 | 3 |
| < 6 | 4 |
A patient with a GCS below 6 receives the maximum SOFA CNS score of 4, which can significantly affect the total SOFA score and the resulting mortality prediction. This makes accurate GCS documentation essential not only for neurological monitoring but also for the integrity of the entire SOFA assessment.
In the original SOFA validation studies, the CNS component (GCS) showed the weakest correlation with mortality compared to the other five organ systems. This is partly because GCS is often confounded by sedation in ICU patients. Despite this, it remains a mandatory SOFA component and must be documented daily for complete severity scoring.
Scoring GCS in Challenging ICU Scenarios
Sedated Patients
Sedation is the most common confounder for GCS assessment in the ICU. A patient on propofol or midazolam may have a GCS of 3 that reflects the drug effect, not neurological injury.
Best practice:
- Record the GCS before sedation is initiated whenever possible
- If sedation is already running, document the GCS with a qualifier: “GCS 6T (on propofol 2 mg/kg/hr)” or “GCS assessed on sedation — not reliable”
- Use a sedation hold (daily awakening trial) to obtain a meaningful GCS when clinically appropriate
- Use the RASS (Richmond Agitation-Sedation Scale) or SAS (Sedation-Agitation Scale) alongside GCS in sedated patients
For SOFA and APACHE II scoring in sedated patients, document the estimated pre-sedation GCS or the GCS obtained during a sedation hold. If neither is available, note this explicitly in the clinical record. A GCS of 3 from sedation should not inflate severity scores in the same way as a GCS of 3 from neurological injury.
Intubated Patients
Endotracheal intubation prevents verbal response assessment. The standard approach is to record the verbal component as “VT” (not testable due to tube) rather than V1.
Some institutions report a modified total as “GCS = E_M_T” (e.g., “GCS = E3M5T = 8T”). Others estimate the verbal component based on the patient’s apparent level of awareness. Either approach is acceptable provided the method is documented consistently.
Patients with Spinal Cord Injury
Patients with high spinal cord injury may be unable to produce motor responses despite intact cortical function. In these cases, use facial motor responses (grimacing to pain) as a substitute and document the limitation clearly.
Patients with Aphasia or Language Barriers
In patients with pre-existing aphasia or in cases where there is a language barrier, the verbal component may be unreliable. Document the limitation and consider whether the patient can follow non-verbal commands (pointing, gesturing) to better assess cognitive function.
Automate GCS tracking across the ICU stay
Rivara Health captures daily GCS assessments as part of your clinical notes and automatically feeds them into SOFA score calculations — so severity documentation is always complete.
Pediatric Glasgow Coma Scale
The standard GCS relies on verbal and motor responses that are not applicable to preverbal children. The Pediatric Glasgow Coma Scale (pGCS) modifies the verbal and motor components for children under 2 years of age.
Pediatric Eye Opening (E): Score 1–4
| Score | Response |
|---|---|
| E4 | Spontaneous |
| E3 | To speech |
| E2 | To pressure |
| E1 | None |
The eye opening component is identical to the adult scale.
Pediatric Verbal Response (V): Score 1–5
| Score | Response |
|---|---|
| V5 | Coos, babbles (age-appropriate vocalisation) |
| V4 | Irritable crying |
| V3 | Cries to pain |
| V2 | Moans to pain |
| V1 | None |
Pediatric Motor Response (M): Score 1–6
| Score | Response |
|---|---|
| M6 | Spontaneous purposeful movement |
| M5 | Localises pain (withdraws to touch) |
| M4 | Normal flexion (withdrawal) |
| M3 | Abnormal flexion |
| M2 | Extension |
| M1 | None |
The pediatric GCS should be used for children under 2 years. For children aged 2–5, use clinical judgement about which scale is more appropriate based on the child’s developmental level. Above age 5, the adult GCS is typically used.
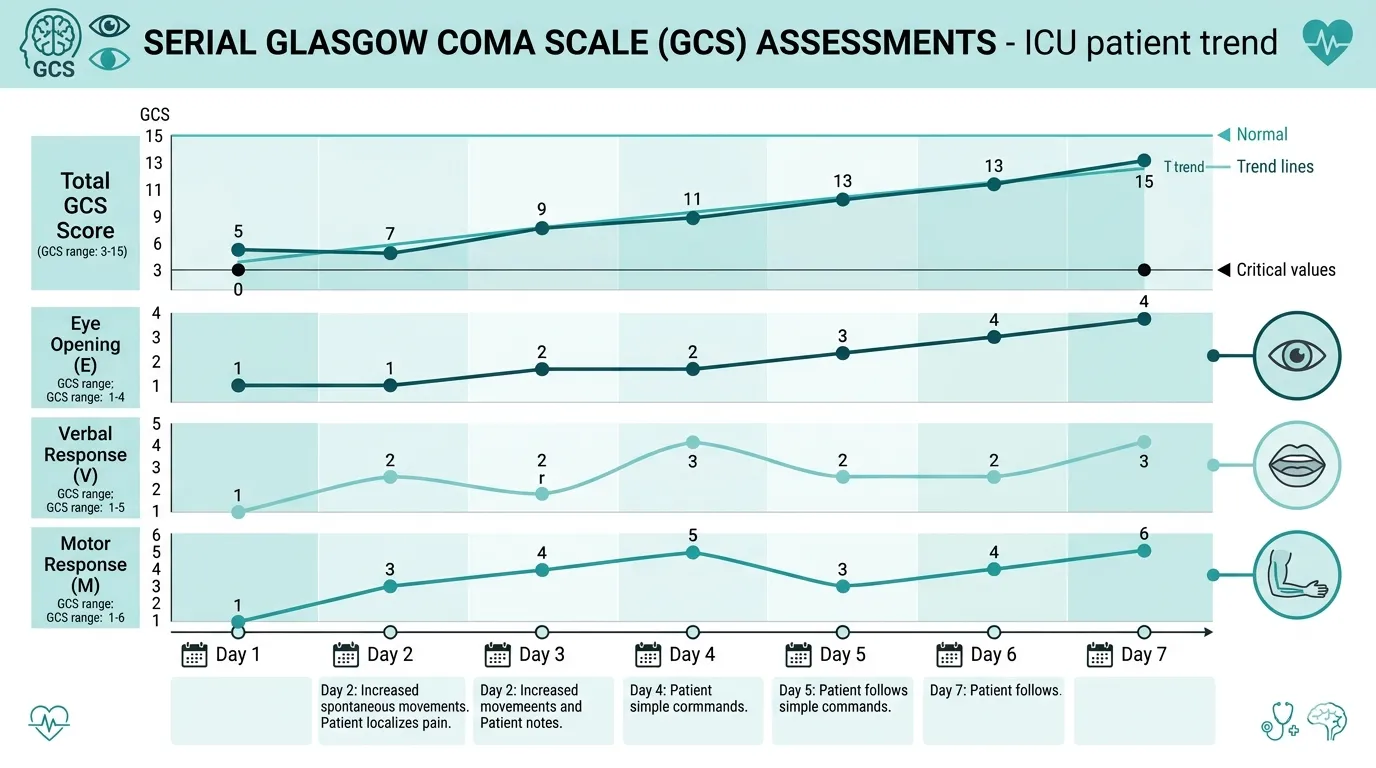
GCS Trends: Why Serial Assessment Matters
A single GCS measurement is a snapshot. The real clinical value of the GCS lies in serial assessments that reveal the trajectory of neurological function over time.
Improving GCS (e.g., 6 on Day 1 → 10 on Day 3 → 13 on Day 5) suggests effective treatment and neurological recovery — supporting continued ICU care and eventual discharge planning.
Deteriorating GCS (e.g., 12 on Day 1 → 9 on Day 2 → 6 on Day 3) signals worsening neurological status and mandates urgent investigation — repeat imaging, escalation of care, or neurosurgical consultation.
Static low GCS (e.g., GCS 4 on Day 1, Day 3, Day 7, Day 14) in the absence of sedation may indicate severe, irreversible brain injury — and becomes an important factor in prognostication discussions with the family and in ICU death summary documentation.
GCS trends are more prognostically valuable than any single GCS value. A patient who arrives with GCS 5 but improves to GCS 10 within 48 hours has a fundamentally different prognosis than one who remains at GCS 5 for a week. Daily GCS documentation captures this trajectory and is essential for both clinical management and complete discharge summary documentation.
GCS in Medicolegal and Insurance Documentation
Why Accurate GCS Documentation Matters
The GCS is one of the most frequently cited clinical parameters in medicolegal proceedings and TPA insurance reviews. It appears in:
- SOFA score calculations that justify ICU-level care
- APACHE II scoring that establishes admission severity
- Intubation decisions — a GCS of 8 or below is the established threshold for airway protection
- Neurosurgical intervention decisions — operative vs conservative management often hinges on GCS
- Prognostication discussions — family meetings about withdrawal of care frequently reference the GCS trajectory
- Death summaries — GCS at admission and the trajectory over the ICU stay are standard elements
Common Documentation Failures
1. Recording total GCS only, without component breakdown. A GCS of “8” in the chart tells the reviewer very little. “E2V2M4” tells them exactly which neurological functions are compromised and allows them to verify that the score was assessed correctly.
2. Failing to note sedation status. A GCS of 3 in a sedated patient is not the same as GCS 3 in an unsedated patient. Without sedation documentation, a TPA reviewer or court may interpret the score as evidence of severe neurological injury when it actually reflected drug effect.
3. Inconsistent timing of assessments. GCS documented at 08:00 one day and 22:00 the next makes trend analysis unreliable. Assess and document at consistent times — ideally tied to nursing shift assessments or daily clinical rounds.
4. Missing GCS in daily notes. If GCS is not documented in the daily clinical note, it cannot be cited for SOFA scoring or severity assessment. Lab values in the system are not sufficient — the GCS must appear in the clinical narrative.
In medicolegal cases, an undocumented GCS is treated as an unassessed GCS. If there is a gap in GCS documentation during a critical period — such as the hours before a patient deteriorated — it creates a documentation void that opposing counsel will exploit. Consistent, timestamped GCS records are your strongest defence.
GCS Quick Reference Card
This summary table consolidates all three components for rapid bedside reference:
| Component | Score 1 | Score 2 | Score 3 | Score 4 | Score 5 | Score 6 |
|---|---|---|---|---|---|---|
| Eye (E) | None | To pressure | To speech | Spontaneous | — | — |
| Verbal (V) | None | Incomprehensible | Inappropriate words | Confused | Oriented | — |
| Motor (M) | None | Extension | Abnormal flexion | Withdrawal | Localises | Obeys commands |
Key thresholds to remember:
- GCS 15 — fully conscious
- GCS ≤ 8 — coma, consider intubation
- GCS 3 — deepest level of unresponsiveness
- Motor score (M) is the single best predictor of outcome among the three components
Your ICU documentation should be as rigorous as your clinical care
Rivara Health generates audit-proof ICU discharge summaries with daily severity scores, neurological assessments, and complete clinical narratives — in under 2 minutes.
7 Practical Tips for GCS Documentation in ICU
-
Always record E + V + M, not just the total. “GCS 9 (E2V3M4)” is clinically useful. “GCS 9” alone is not.
-
Note the stimulus used. “GCS assessed with trapezius squeeze” or “GCS assessed with verbal command” clarifies the assessment method and reproducibility.
-
Document sedation status alongside every GCS. “GCS 5T on propofol 3 mg/kg/hr” versus “GCS 5 off sedation for 4 hours” — these are fundamentally different clinical scenarios.
-
Use “NT” (not testable) for components that cannot be assessed. Swollen eyes = E(NT). Intubated = V(T). Spinal cord injury = M(NT). Never assign a score of 1 when the component is physically untestable.
-
Assess at consistent times. Tie GCS assessment to daily clinical rounds or nursing shift changes. Consistency enables meaningful trend analysis.
-
Record the best response observed. If the patient opens eyes spontaneously at one point during the assessment but not at another, score E4 (the best response). The GCS captures maximal capability, not average behaviour.
-
Reassess after any clinical change. New seizure activity, a sedation hold, post-operative return, or any acute deterioration should trigger a fresh GCS assessment, documented with a timestamp.
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Conclusion
The Glasgow Coma Scale remains the global standard for neurological assessment in the ICU more than five decades after its introduction. Its simplicity is its strength — three components, each independently scored, producing a total that is universally understood by clinicians, nurses, insurance reviewers, and courts.
But simplicity does not mean the GCS is simple to document correctly. Sedation, intubation, spinal cord injury, and language barriers all confound the assessment. The difference between M4 and M5, or the failure to note “VT” in an intubated patient, can cascade into inaccurate SOFA scores, misleading severity assessments, and weakened medicolegal records.
For ICU clinicians, the standard is clear: document GCS as E + V + M with the total, note the sedation status and any confounders, assess at consistent intervals, and ensure the GCS appears in daily clinical notes — not just nursing charts.
Tools like Rivara Health’s ICU Summary Generator integrate daily GCS assessments into structured clinical notes and automatically calculate the resulting SOFA score, ensuring that neurological documentation is complete, consistent, and audit-ready from admission through to the discharge summary.
Related reading: SOFA Score in ICU: Complete Guide for Clinicians | Complete Guide to ICU Discharge Summaries | ICU Death Summary Guide
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Reduce ICU Documentation Time by 90%
Generate medicolegal-grade ICU discharge summaries in under 2 minutes. Built for Indian hospitals, designed for TPA compliance.