The Sequential Organ Failure Assessment (SOFA) score is the standard severity scoring system in intensive care medicine. It assesses the function of 6 organ systems, assigning a score of 0–4 for each, yielding a total score of 0–24.
In ICU practice, the SOFA score serves three critical purposes: it guides clinical decision-making, justifies the intensity of ICU care to TPA insurance companies, and is increasingly cited in medicolegal proceedings as evidence of illness severity.
This guide covers SOFA score calculation across all 6 components, how to interpret the scores clinically, and how to document them effectively for insurance and medicolegal purposes.

What Is the SOFA Score?
Developed in 1994 by the European Society of Intensive Care Medicine, the SOFA score was originally called the Sepsis-related Organ Failure Assessment. It was later renamed Sequential Organ Failure Assessment to reflect its broader utility beyond sepsis.
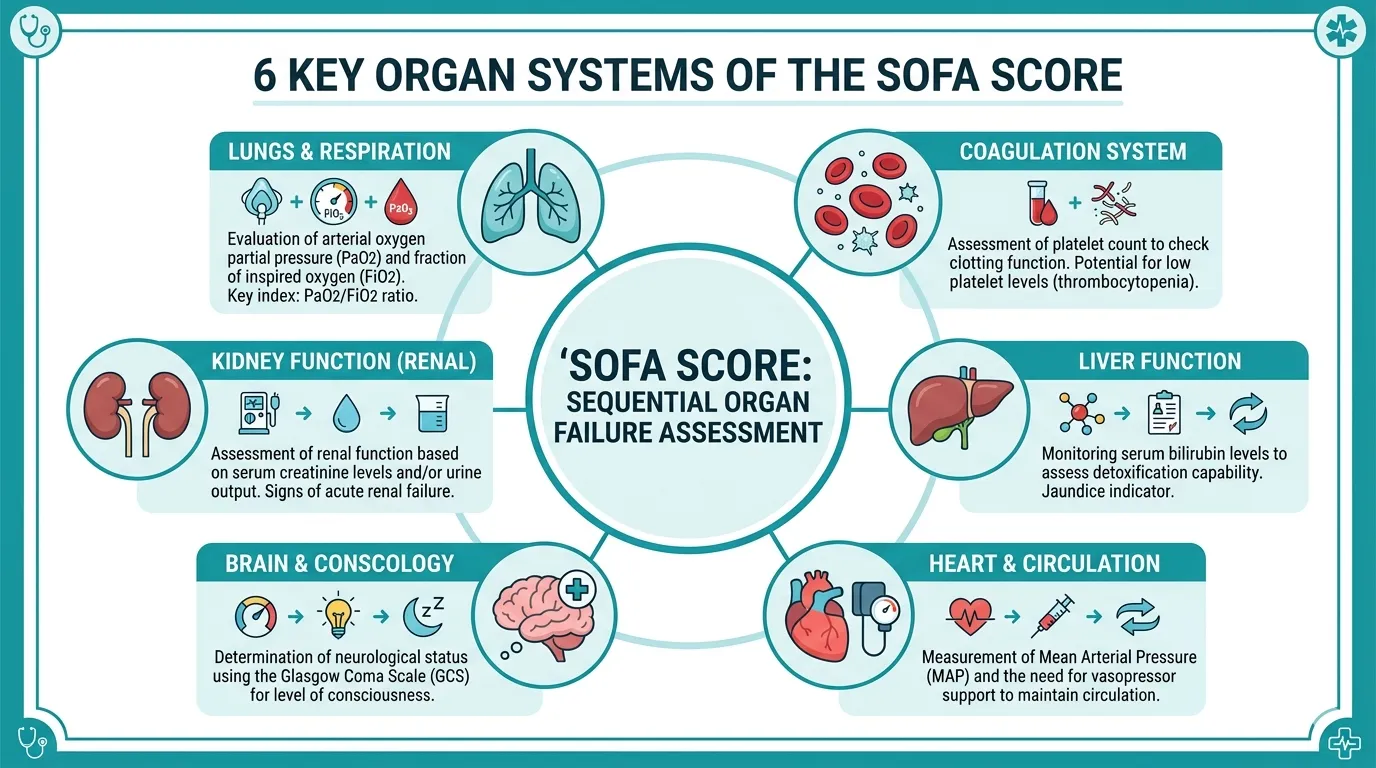
The score assesses 6 organ systems, each scored from 0 (normal) to 4 (severe dysfunction):
- Respiratory — PaO₂/FiO₂ ratio
- Coagulation — Platelet count
- Hepatic — Bilirubin
- Cardiovascular — Mean arterial pressure and vasopressor requirements
- Central Nervous System — Glasgow Coma Scale
- Renal — Creatinine and urine output
The maximum total score is 24. Higher scores correspond directly to higher predicted mortality — making accurate, daily SOFA documentation critical for both clinical and administrative purposes.
SOFA Score: Component-by-Component Guide
1. Respiratory Component (PaO₂/FiO₂ Ratio)
The respiratory component reflects gas exchange efficiency, measured as the ratio of arterial oxygen partial pressure (PaO₂) to the fraction of inspired oxygen (FiO₂).
| PaO₂/FiO₂ Ratio | SOFA Score |
|---|---|
| ≥ 400 | 0 — normal |
| 300–399 | 1 |
| 200–299 | 2 |
| 100–199 (with ventilatory support) | 3 |
| < 100 (with ventilatory support) | 4 |
In patients breathing room air (FiO₂ = 0.21), a normal PaO₂ of 100 mmHg gives a P/F ratio of ~476, well within normal. A P/F ratio below 300 indicates acute lung injury; below 200 indicates ARDS.
Always document the FiO₂ alongside PaO₂ in daily notes. Without FiO₂, the P/F ratio cannot be calculated. Many TPA disputes arise specifically from missing FiO₂ documentation.
2. Coagulation Component (Platelet Count)
Platelet count reflects coagulopathy, which is common in sepsis, liver failure, and disseminated intravascular coagulation (DIC).
| Platelet Count (×10³/µL) | SOFA Score |
|---|---|
| ≥ 150 | 0 — normal |
| 100–149 | 1 |
| 50–99 | 2 |
| 20–49 | 3 |
| < 20 | 4 |
A rapidly declining platelet count is often more clinically significant than the absolute value. A count falling from 180 to 60 over 48 hours tells a different story than a stable count of 60. Document the trend in your daily notes.
Log platelet counts from daily CBCs in the ICU notes. Do not rely on the lab report alone — it must be in the clinical notes for SOFA scoring. TPA reviewers check for the source value, not just the derived score.
3. Hepatic Component (Bilirubin)
The hepatic component uses total bilirubin to assess liver dysfunction.
| Bilirubin (mg/dL) | SOFA Score |
|---|---|
| < 1.2 | 0 — normal |
| 1.2–1.9 | 1 |
| 2.0–5.9 | 2 |
| 6.0–11.9 | 3 |
| ≥ 12.0 | 4 |
Differentiate between direct and indirect hyperbilirubinaemia. Sepsis typically causes a mixed picture. Pre-existing liver disease (cirrhosis, hepatitis) inflates this score even in the absence of new hepatic failure.
Note pre-existing baseline bilirubin on admission where available. A TPA reviewer seeing a bilirubin SOFA score of 3–4 may question whether it reflects acute ICU illness or a pre-existing condition — baseline documentation protects you.
4. Cardiovascular Component (MAP and Vasopressors)
The cardiovascular component is the most complex, incorporating both mean arterial pressure (MAP) and vasopressor requirements.
| Cardiovascular Status | SOFA Score |
|---|---|
| MAP ≥ 70 mmHg | 0 |
| MAP < 70 mmHg | 1 |
| Dopamine ≤ 5 µg/kg/min OR Dobutamine (any dose) | 2 |
| Dopamine > 5 µg/kg/min OR Norepinephrine ≤ 0.1 µg/kg/min OR Epinephrine ≤ 0.1 µg/kg/min | 3 |
| Dopamine > 15 µg/kg/min OR Norepinephrine > 0.1 µg/kg/min OR Epinephrine > 0.1 µg/kg/min | 4 |
Vasopressor dose matters enormously for TPA claims. An ICU patient on norepinephrine > 0.1 µg/kg/min (SOFA cardiovascular 4) requires a completely different level of nursing care and monitoring than one requiring no vasopressors — and TPA reviewers know this.
Document exact vasopressor doses and timing. “Patient was on vasopressors” is insufficient. “Norepinephrine 0.12 µg/kg/min at 08:00, titrated down to 0.06 µg/kg/min by 20:00” is what is needed for TPA review.
5. CNS Component (Glasgow Coma Scale)
The central nervous system component uses the Glasgow Coma Scale (GCS).
| GCS | SOFA Score |
|---|---|
| 15 | 0 — normal |
| 13–14 | 1 |
| 10–12 | 2 |
| 6–9 | 3 |
| < 6 | 4 |
In sedated patients, the GCS is confounded by sedation. Document whether the GCS was recorded off sedation, on sedation, or represents a best-estimate. Many units use RASS (Richmond Agitation-Sedation Scale) for sedated patients — note this separately.
Record GCS with component breakdown (E + V + M = total) rather than just the total. A GCS of 8 could be E2V2M4 (very different from E4V1M3) — the breakdown matters both clinically and medicolegally.
6. Renal Component (Creatinine and Urine Output)
The renal component incorporates both serum creatinine and urine output. The higher scoring criterion takes precedence.
| Creatinine (mg/dL) / Urine Output | SOFA Score |
|---|---|
| Creatinine < 1.2 | 0 |
| Creatinine 1.2–1.9 | 1 |
| Creatinine 2.0–3.4 | 2 |
| Creatinine 3.5–4.9 OR urine output < 500 mL/day | 3 |
| Creatinine ≥ 5.0 OR urine output < 200 mL/day | 4 |
Both creatinine and urine output are included — the higher score takes precedence. A patient with creatinine of 2.5 (score 2) but oliguria < 500 mL/day scores a 3, not a 2. Miss this and you will understate illness severity.
Document 24-hour urine output in every daily note, not just the most recent value. Trends in urine output are critical for assessing AKI progression and response to treatment — and are frequently scrutinised in TPA disputes.
Stop calculating SOFA scores manually
Rivara Health automatically computes SOFA scores from your daily note entries — across all 6 components, every day of the ICU stay.
Interpreting the Total SOFA Score
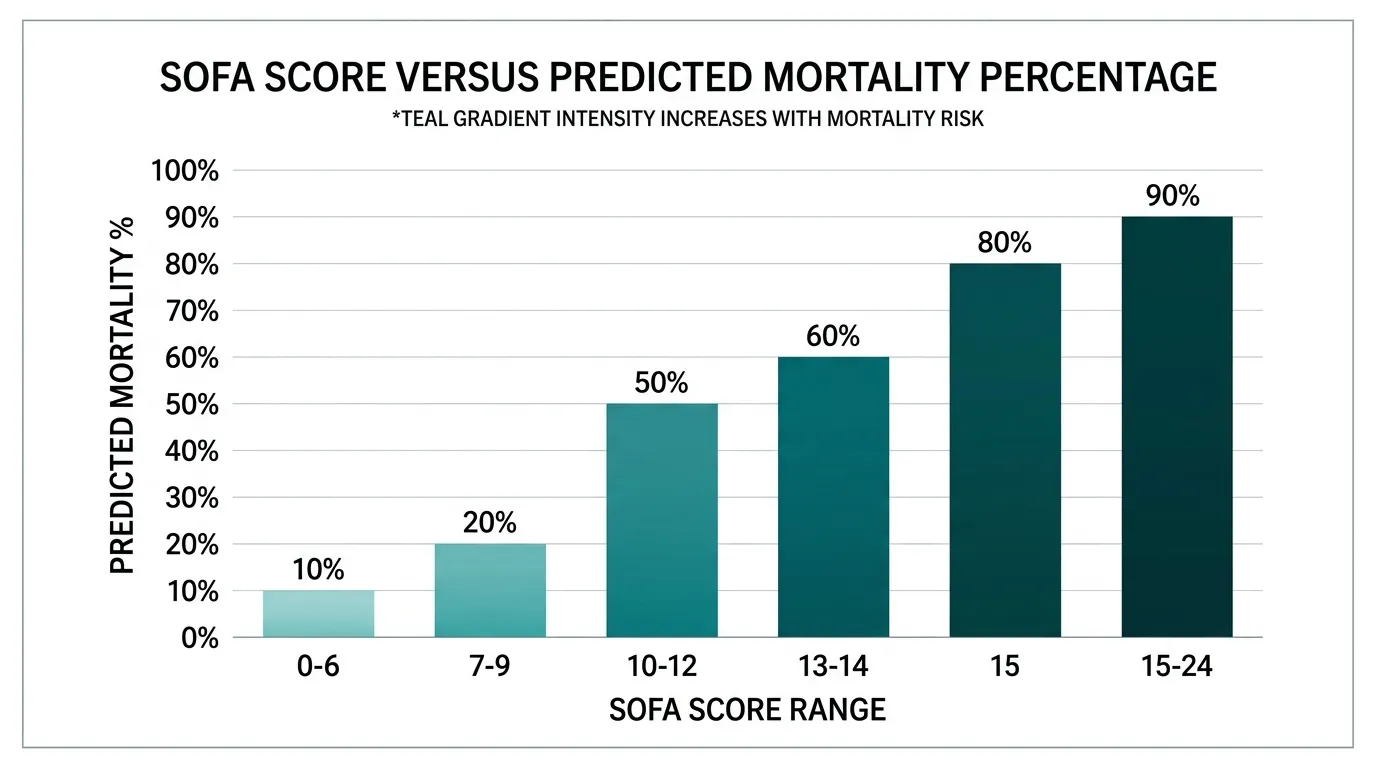
| Total SOFA Score | Predicted Mortality |
|---|---|
| 0–6 | < 10% |
| 7–9 | 15–20% |
| 10–12 | 40–50% |
| 13–14 | 50–60% |
| 15 | > 80% |
| 15–24 | > 90% |
These are population-level predictions based on the original SOFA validation cohorts. Individual patient outcomes depend on age, comorbidities, cause of ICU admission, quality of care, and time to intervention. Use as a severity indicator, not a guarantee.
For TPA and medicolegal purposes, a SOFA score of 10 or above is widely recognised as indicating critical illness with high mortality risk — justifying the full resources of ICU care.
SOFA Score and TPA Insurance Claims in India
Insurance reviewers use SOFA scores as part of their assessment of whether the level of ICU care claimed was clinically appropriate. A patient with a peak SOFA score of 3 throughout a 10-day ICU stay may face more scrutiny than one with scores consistently above 10.
What TPA reviewers look for:
- Daily SOFA scores — not just admission and discharge values
- Trend over time — worsening scores justify escalation of care; improving scores reflect response to treatment
- Component documentation — each component must be traceable to a documented lab value or clinical finding
- Correlation with interventions — a SOFA cardiovascular score of 4 should correlate with documented vasopressor doses
Common TPA rejection triggers related to SOFA:
- SOFA scores claimed without supporting lab values in the notes
- Cardiac SOFA scores not matched by vasopressor documentation
- CNS SOFA scores inconsistent with nursing observation notes
- No daily SOFA documentation — only admission and discharge values
A claim rejected due to inadequate SOFA documentation is almost always preventable. The data exists in the lab reports and nursing charts — the problem is that it was never consolidated into the daily clinical note in a format the TPA can verify.
Is poor SOFA documentation costing you TPA approvals?
Rivara Health generates audit-proof ICU discharge summaries with daily SOFA scores, component-level documentation, and linked lab values — in under 2 minutes.
How Rivara Health Handles SOFA Scoring
Rivara Health’s ICU Summary Generator automatically calculates the SOFA score from the values entered in each daily note. Doctors enter the relevant lab values and clinical parameters, and the app computes the total SOFA score and each component score.
The scores are tracked across the entire ICU stay, creating a graph of disease severity over time. When the AI generates the discharge summary, it references the SOFA score trajectory as part of the clinical narrative — providing exactly the kind of documentation TPA reviewers and courts expect.
This means doctors never need to manually calculate SOFA scores. The math is done automatically, and the scores are embedded in the clinical record with the lab values that support them.
6 Practical Tips for SOFA Documentation
-
Enter lab values, not just SOFA scores. The score should always be derivable from documented values. Never enter a SOFA score without the supporting PaO₂/FiO₂, platelet count, bilirubin, creatinine, and GCS.
-
Document vasopressor doses with units. “Noradrenaline 6 mL/hr” is meaningless without knowing the concentration. Document in µg/kg/min.
-
Record 24-hour urine output every day. This is the most commonly missing value in renal SOFA documentation.
-
Note GCS component breakdown. E + V + M, not just the total.
-
Flag pre-existing organ dysfunction. If a patient has baseline CKD with creatinine of 2.0, note this on admission. A creatinine of 2.5 in this patient represents less acute deterioration than in a patient with previously normal kidneys.
-
Calculate SOFA at the same time each day. Consistency in timing reduces variability and makes trends more interpretable.
Conclusion
The SOFA score is one of the most powerful tools in ICU medicine — both clinically and from a documentation standpoint. Proper SOFA scoring requires accurate, daily documentation of 6 specific physiological parameters, each traceable to an objective measurement.
For ICU doctors, systematic SOFA documentation is not optional — it is essential for insurance claim approval and medicolegal protection.
Tools like Rivara Health’s ICU Summary Generator automate SOFA calculation and embed it in daily clinical notes, ensuring that the documentation meets the standards required by TPA companies and courts — without adding meaningfully to the doctor’s workload.
Learn more about how AI is transforming ICU discharge documentation in India, or explore the ICU discharge summary generator to see how it works in practice.
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Reduce ICU Documentation Time by 90%
Generate medicolegal-grade ICU discharge summaries in under 2 minutes. Built for Indian hospitals, designed for TPA compliance.