The ICU discharge summary is the single most important document produced during a patient’s intensive care stay. It synthesises days or weeks of complex clinical data — ventilator settings, vasopressor titrations, laboratory trends, procedures, complications — into a coherent narrative that follows the patient beyond the ICU. This discharge summary guide covers everything an intensivist needs to produce documentation that is clinically useful, legally defensible, and administratively complete.
Whether you are a senior consultant or a resident writing your first ICU discharge summary, the principles are the same: accuracy, completeness, and clinical reasoning made visible on paper.

What Is an ICU Discharge Summary?
An ICU discharge summary is a structured clinical document that captures the complete narrative of a patient’s ICU stay — from the reason for admission through the clinical course, interventions, complications, and final outcome — along with a plan for ongoing care.
It differs from a ward discharge summary in several important ways:
| Feature | Ward Discharge Summary | ICU Discharge Summary |
|---|---|---|
| Clinical complexity | Single or few diagnoses | Multi-organ involvement, multiple concurrent therapies |
| Temporal detail | Summary of stay | Day-by-day or phase-by-phase clinical course |
| Procedures | Minor, if any | Intubation, central lines, dialysis, chest drains, surgeries |
| Medication complexity | Standard regimens | Vasopressors with dose titrations, sedation protocols, antibiotic escalation/de-escalation |
| Severity scoring | Rarely included | SOFA, APACHE II, GCS documented serially |
| Handoff complexity | Single receiving team | Multiple: ward team, rehabilitation, outpatient, primary care |
The ICU discharge summary is not just a medical record — it is a clinical handoff tool, a legal document, an insurance submission, and a quality metric artefact, all in one.
The discharge summary is often the only document that a downstream physician — whether a ward consultant, a rehabilitation specialist, or a primary care doctor — will read about the ICU stay. If it is incomplete, the receiving team is flying blind. If it is inaccurate, clinical decisions downstream may be wrong.
Why ICU Discharge Summaries Matter
Continuity of Care
ICU patients are among the most complex in any hospital. When they transition to a step-down unit, general ward, or another facility, the receiving team inherits a patient with multiple active problems, ongoing medication requirements, and specific monitoring needs. The discharge summary is how this clinical context transfers.
A study published in Critical Care Medicine found that incomplete ICU discharge documentation was associated with a 24% increase in adverse events within 72 hours of ICU transfer. The most common gaps were incomplete medication reconciliation and missing follow-up instructions.
Legal and Medicolegal Protection
In malpractice proceedings and coroner inquiries, the discharge summary is frequently the first document reviewed. Courts and medical boards assess whether the documented care met the standard expected of a reasonable intensivist. Gaps in documentation are interpreted unfavourably — not as “it wasn’t documented” but as “it wasn’t done.”
The legal standard is simple: if it isn’t documented, it didn’t happen. A procedure you performed but didn’t record, a complication you managed but didn’t note, a family discussion you had but didn’t write down — none of these exist in the medicolegal record. The discharge summary is your evidence.
Insurance and Reimbursement
Insurance companies and third-party administrators (TPAs) use discharge summaries to determine the appropriateness and extent of ICU care provided. Inadequate documentation is one of the leading causes of claim denials globally. Key elements that insurers scrutinise include:
- Medical necessity for ICU admission
- Justification for length of stay
- Documentation of procedures and their indications
- Severity scores supporting the level of care
For a detailed guide on insurance-specific documentation requirements, see our guide to ICU discharge summaries for TPA insurance documentation.
Quality Metrics and Benchmarking
ICU discharge summaries feed into hospital quality programmes, national registries, and benchmarking databases. Accurate documentation of diagnoses, procedures, severity scores, and outcomes determines how your unit is measured against peers — and affects accreditation, funding, and resource allocation.
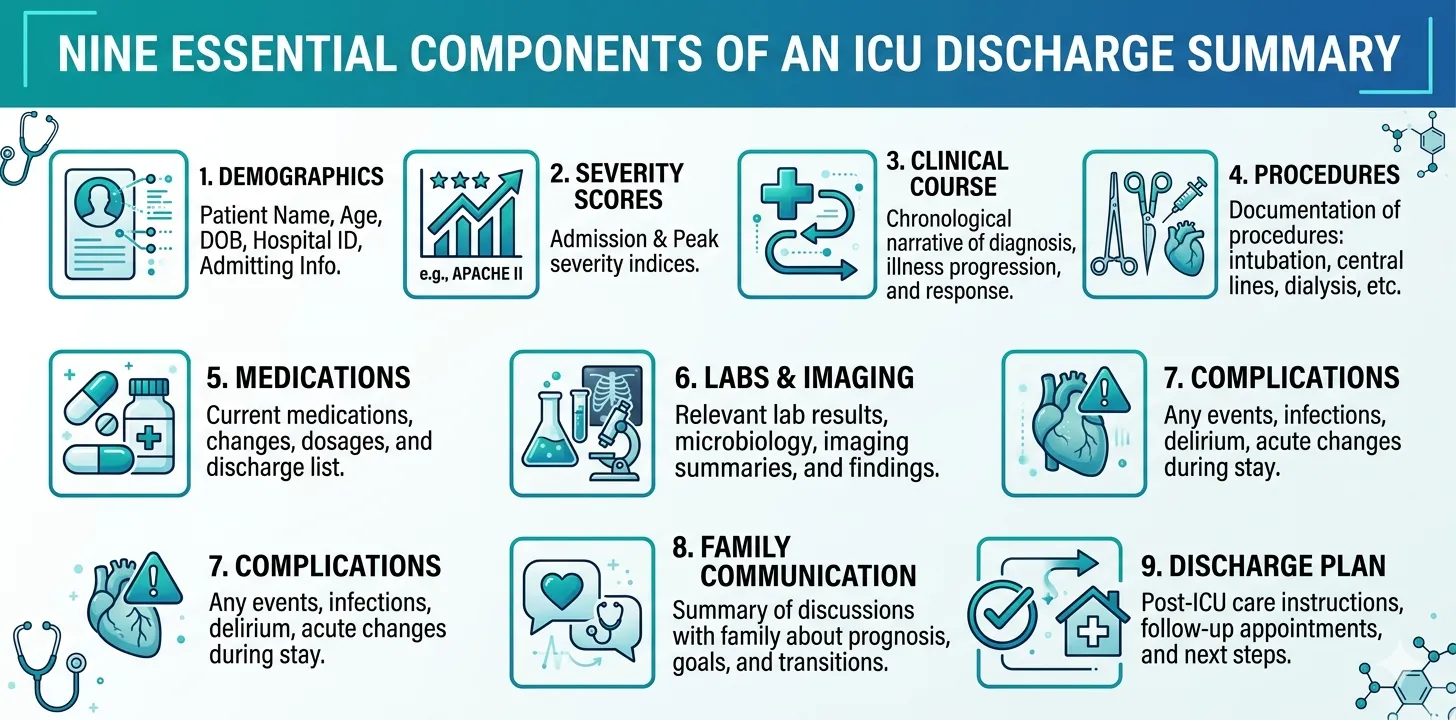
Essential Components of an ICU Discharge Summary
Every ICU discharge summary, regardless of institution or country, must cover the following elements. The level of detail will vary by patient complexity and local requirements, but omitting any section entirely creates documentation gaps that can have clinical, legal, or financial consequences.
1. Patient Demographics and Admission Details
This section establishes the baseline:
- Patient identifiers: Name, age, sex, medical record number
- Date and time of ICU admission (and hospital admission if different)
- Source of admission: Emergency department, operating theatre, ward transfer, inter-hospital transfer
- Admitting diagnosis: The primary reason for ICU admission, stated clearly
- Indication for ICU-level care: Why this patient needed intensive care rather than ward-level monitoring
- Relevant comorbidities: Pre-existing conditions that affect the ICU course (diabetes, CKD, COPD, immunosuppression, etc.)
- Baseline functional status: Pre-illness functional capacity, mobility, cognitive status
State the ICU admission indication explicitly. “Admitted for monitoring” is insufficient. “Admitted for invasive mechanical ventilation and vasopressor support in the setting of septic shock secondary to community-acquired pneumonia” establishes medical necessity unambiguously.
2. Severity Scores at Admission
Severity scoring provides an objective, reproducible measure of illness severity at the time of ICU admission. The two most widely used systems are:
SOFA Score (Sequential Organ Failure Assessment)
- Scored across 6 organ systems (respiratory, coagulation, hepatic, cardiovascular, CNS, renal)
- Range: 0–24
- Provides both a snapshot of severity and, when scored daily, a trajectory of organ function
For a component-by-component breakdown with reference ranges and scoring tables, see our complete SOFA score guide for ICU clinicians.
APACHE II Score (Acute Physiology and Chronic Health Evaluation)
- Calculated from 12 physiological variables, age, and chronic health status within the first 24 hours of ICU admission
- Range: 0–71
- Widely used for benchmarking and mortality prediction
For a detailed APACHE II walkthrough, see our APACHE II score guide.
| Scoring System | When to Calculate | Components | Primary Use |
|---|---|---|---|
| SOFA | Admission + daily | 6 organ systems | Organ dysfunction tracking, daily severity assessment |
| APACHE II | First 24 hours only | 12 physiology variables + age + chronic health | Admission severity, mortality prediction, benchmarking |
Include the raw values that generated the scores, not just the final number. An admission SOFA of 12 means nothing to a downstream clinician without knowing which organ systems were failing. “SOFA 12 (Resp 3, Coag 1, Hepatic 0, Cardio 4, CNS 2, Renal 2)” tells the clinical story.
3. Clinical Course
The clinical course is the narrative backbone of the discharge summary. It describes what happened between admission and discharge — the patient’s trajectory, treatment decisions, response to therapy, and complications encountered.
For short ICU stays (1–3 days), a chronological narrative is usually sufficient. For longer stays, organise the course by clinical phase rather than day-by-day, to maintain readability:
Example structure for a 14-day ICU stay:
- Days 1–3: Initial resuscitation and stabilisation. Septic shock requiring norepinephrine up to 0.3 µg/kg/min. Intubated for hypoxaemic respiratory failure (P/F ratio 110). Empiric antibiotics initiated (piperacillin-tazobactam + vancomycin). Blood cultures grew E. coli.
- Days 4–7: Organ support and source control. CT abdomen revealed perforated diverticulitis. Emergency laparotomy performed on Day 4. Vasopressors weaned by Day 6. Antibiotics narrowed to ceftriaxone based on sensitivities.
- Days 8–11: Ventilator weaning. Transitioned from volume-control to pressure support ventilation. Failed initial SBT on Day 8 (tachypnoea, accessory muscle use). Successful SBT and extubation on Day 10. Developed post-extubation stridor managed with nebulised adrenaline and dexamethasone.
- Days 12–14: Step-down and discharge preparation. Transferred to high-flow nasal cannula. Oral diet resumed. Physiotherapy initiated. Discharged to surgical ward on Day 14.
Write the clinical course as a narrative that a colleague could read and understand the patient’s trajectory without accessing any other records. Avoid bullet-point lists of daily events — synthesise them into a clinical story with cause-and-effect reasoning visible.
4. Procedures and Interventions
Every procedure performed during the ICU stay must be documented with:
- Procedure name (use standard terminology)
- Date and time
- Indication
- Operator (or supervised trainee)
- Outcome and any complications
Common ICU procedures that must be documented:
| Procedure | Key Details to Include |
|---|---|
| Endotracheal intubation | Route (oral/nasal), tube size, grade of view, number of attempts, drugs used |
| Central venous catheter | Site (IJ, subclavian, femoral), laterality, confirmation method (USS, CXR), complications |
| Arterial line | Site, laterality, confirmation |
| Mechanical ventilation | Mode, key settings (PEEP, FiO₂, tidal volume), duration |
| Tracheostomy | Surgical vs percutaneous, tube size, date, complications |
| Chest drain / intercostal tube | Side, indication, output |
| Renal replacement therapy | Modality (CRRT, IHD), duration, access, indication |
| Bronchoscopy | Indication, findings, any therapeutic intervention |
| Lumbar puncture | Opening pressure, CSF findings |
| Blood product transfusions | Product type, units, indication, any reactions |
Undocumented procedures are a leading source of medicolegal risk. If a central line was inserted and later the patient develops a line-related bloodstream infection, the documentation of the insertion — technique, sterile precautions, site selection rationale — becomes critical evidence. Document at the time of the procedure, not retrospectively.
5. Medications and Therapeutic Agents
ICU medication documentation requires more detail than standard ward prescriptions because of the clinical significance of dose titrations, duration, and sequencing:
Critical categories to document:
- Vasopressors and inotropes: Agent, peak dose (in µg/kg/min), duration, weaning trajectory
- Sedation and analgesia: Agents, infusion rates, any sedation scoring (RASS), neuromuscular blockade if used
- Antimicrobials: Each antibiotic/antifungal, dose, duration, indication, culture and sensitivity data, escalation/de-escalation decisions with rationale
- Anticoagulation: Agent, dose, indication, monitoring (anti-Xa, aPTT, INR), any bleeding events
- Nutrition: Route (enteral vs parenteral), target and achieved caloric intake, any GI intolerance
- Significant medications at discharge: What the patient is leaving on, with dose, route, frequency, and intended duration
Spending hours reconstructing medication histories at discharge?
Rivara Health captures medications, vasopressor doses, and antibiotic timelines as part of daily ICU notes — so the discharge summary writes itself.
6. Laboratory and Investigation Results
Include key laboratory trends, not every individual result. The goal is to communicate the trajectory of organ function:
- Admission baseline labs: CBC, metabolic panel, coagulation, lactate, blood gas
- Key trends: Rising creatinine indicating AKI, falling platelets suggesting DIC, improving lactate clearance
- Culture and sensitivity results: All positive cultures with organisms and resistance patterns
- Imaging findings: Key radiological findings (CXR, CT, ultrasound) with dates
- Special investigations: Echocardiography findings, EEG if relevant, histopathology results
Avoid copying entire lab panels into the discharge summary. A table showing admission, peak, and discharge values for key parameters (creatinine, bilirubin, lactate, platelets, WBC) communicates more effectively than pages of daily results.
7. Complications
Every complication that occurred during the ICU stay must be documented, along with how it was identified and managed:
- Ventilator-associated pneumonia (VAP)
- Central line-associated bloodstream infection (CLABSI)
- Acute kidney injury (AKI) — staging per KDIGO criteria
- Delirium — duration, management
- Pressure injuries
- Unplanned extubation or reintubation
- Drug adverse reactions
- Thromboembolic events
Document complications objectively. Avoid defensive language (“despite best efforts”) — state what happened, when, how it was detected, and what was done. Factual documentation is stronger medicolegal protection than defensive prose.
8. Family Communication and Shared Decision-Making
Document all significant family discussions, including:
- Prognosis discussions: What was communicated, who was present, family’s understanding
- Goals of care: Full escalation, limitations of treatment, comfort care decisions
- Consent: For procedures, for withdrawal of treatment if applicable
- Advance directives: Any existing directives and how they were incorporated into care
Documentation of family communication protects the treating team in two ways: it demonstrates that the family was informed and involved in decision-making, and it creates a contemporaneous record of what was discussed — which is stronger evidence than any later recollection.
9. Discharge Condition and Follow-Up Plan
The discharge section must clearly state:
- Condition at ICU discharge: Vital signs, consciousness level, respiratory status (room air vs supplemental O₂), functional status
- Active problems at discharge: What remains unresolved
- Medications at discharge: Complete list with dose, route, frequency, intended duration
- Pending results: Cultures, biopsies, or investigations still awaited
- Follow-up plan: Specific follow-up appointments, investigations needed, parameters to monitor
- Red flags for readmission: Specific clinical signs that should prompt ICU review or readmission
- Receiving team handoff: Name and contact of the accepting physician/team
Step-by-Step Guide to Writing an ICU Discharge Summary
Writing an ICU discharge summary does not need to take hours — if the right data has been collected during the stay. Here is a systematic approach:
Step 1: Gather Your Sources
Before writing a single word, assemble:
- Daily ICU progress notes
- Procedure notes
- Nursing charts (fluid balance, ventilator records, vasopressor sheets)
- Laboratory reports (with culture results)
- Imaging reports
- Consultant notes (surgery, nephrology, neurology, etc.)
- Family meeting notes
Step 2: Establish the Narrative Arc
Every ICU stay has a clinical narrative arc. Identify it before you start writing:
- Why was the patient admitted? (Presenting problem and diagnosis)
- What went wrong? (Organ failures, complications)
- What did we do? (Interventions, procedures, therapies)
- How did the patient respond? (Improvement, deterioration, plateau)
- Where is the patient now? (Discharge condition)
- What happens next? (Follow-up plan)
This arc keeps your summary focused and readable, even for complex 20-day stays.
Step 3: Write the Admission Section
Start with demographics, admission date, source, diagnosis, and indication for ICU care. Include admission severity scores with component-level detail. State relevant comorbidities and baseline functional status.
Step 4: Write the Clinical Course
Use the phase-based approach for stays longer than 3 days. Each phase should cover:
- The clinical problem at that phase
- The key interventions
- The patient’s response
- Any complications that emerged
Step 5: Document Procedures, Medications, and Investigations
These can be structured as tables or lists. Prioritise completeness over prose — this is reference material, not narrative.
Step 6: Document Complications and Family Communication
Be factual and specific. Date and time every significant event and conversation.
Step 7: Write the Discharge Plan
This is arguably the most actionable section. The receiving team will use it to guide immediate management. Be specific: which medications, which investigations, which parameters to monitor, and what should trigger an ICU review.
Step 8: Review and Finalise
Before signing off, verify:
- All procedures are documented
- Medication list is complete and current
- Severity scores are included with source values
- Culture results and antibiotic decisions are documented
- Complications are listed with management
- Discharge medications match the patient’s current regimen
- Follow-up plan is specific and actionable
- Pending results are flagged
Common Mistakes and How to Avoid Them
Even experienced intensivists make documentation errors — often not from lack of knowledge, but from time pressure and workflow friction. Here are the most consequential mistakes:
Mistake 1: Vague Admission Indications
Poor: “Admitted to ICU for monitoring.”
Better: “Admitted to ICU for invasive mechanical ventilation and vasopressor support in the setting of community-acquired pneumonia complicated by septic shock (SOFA 14, APACHE II 28).”
The vague version fails to establish medical necessity. The detailed version makes the case for ICU-level care immediately clear.
Mistake 2: Missing or Incomplete Severity Scores
Stating “SOFA score: 12” without component breakdown is nearly as unhelpful as omitting it. Always include individual organ system scores and the raw values that generated them.
Mistake 3: Copy-Paste Clinical Course
Copying daily progress notes verbatim into the clinical course produces an unreadable wall of text. The discharge summary should synthesise and interpret, not duplicate. A 15-day ICU stay should yield a clinical course of 4–6 paragraphs organised by phase — not 15 paragraphs of copy-pasted daily notes.
Mistake 4: Undocumented Medication Changes
Antibiotic escalation without a documented rationale, vasopressor dose changes without timing, sedation adjustments without a RASS target — these gaps create both clinical and legal vulnerability. Every significant medication change should include the reason.
Mistake 5: No Complication Documentation
Omitting complications does not protect you — it exposes you. If a VAP or CLABSI occurred and was managed appropriately but not documented, you have no evidence that you identified and treated it. Downstream complications from unacknowledged events become indefensible.
Mistake 6: Generic Follow-Up Plans
Poor: “Follow up in OPD.”
Better: “Follow up with pulmonology in 2 weeks for repeat spirometry and assessment of supplemental oxygen requirements. Repeat renal function tests in 1 week — if creatinine rises above 2.0 mg/dL, refer to nephrology. Surgical wound review in 10 days with general surgery.”
A useful test for your follow-up plan: could a doctor who has never seen this patient execute it without calling you? If the answer is no, add more detail.
Mistake 7: Delayed Documentation
Writing the discharge summary days or weeks after the patient has left the ICU introduces recall bias, omissions, and inaccuracies. The summary should be completed within 24 hours of ICU discharge — ideally before the patient physically transfers.
| Mistake | Risk | Fix |
|---|---|---|
| Vague admission indication | Insurance denial, medicolegal exposure | State diagnosis + indication + severity scores |
| Missing severity scores | Cannot benchmark, insurance queries | Include SOFA/APACHE with components |
| Copy-paste clinical course | Unreadable, misses clinical reasoning | Synthesise by phase, show cause-and-effect |
| Undocumented medication changes | Legal risk, continuity failures | Document every change with rationale and timing |
| Omitted complications | No evidence of appropriate management | Document factually: event, detection, management |
| Generic follow-up plan | Downstream care failures | Be specific: who, when, what, and triggers for escalation |
| Delayed documentation | Recall bias, inaccuracies | Complete within 24 hours of ICU discharge |
Documentation Standards and Best Practices
Timeliness
The Joint Commission, NHS England, the Australian Commission on Safety and Quality, and most national accreditation bodies require discharge summaries to be completed within 24–48 hours of discharge. In practice, ICU discharge summaries should be completed before or at the time of transfer.
Structured vs. Free-Text
Structured templates improve completeness and reduce omissions. A study in the Journal of Critical Care found that structured discharge templates reduced documentation gaps by 40% compared to free-text summaries.
Use a template that includes mandatory fields for each of the essential components listed above. Free-text narrative is appropriate for the clinical course section; every other section benefits from structured data entry.
Standardised Terminology
Use standard medical terminology consistently:
- ICD codes for diagnoses where required
- Standard procedure nomenclature
- Drug names (generic, not brand) with standardised dosing units
- Severity scores calculated per published criteria
Signature and Accountability
The discharge summary should identify:
- The author (the physician who wrote the summary)
- The attending intensivist (who supervised the patient’s care)
- The date and time the summary was completed
Many malpractice cases hinge on the question “Who was responsible for this patient’s care?” A clearly attributed discharge summary — with named author and supervising physician — establishes the chain of responsibility and demonstrates accountability.
Structured daily notes that build your discharge summary automatically
Rivara Health collects structured clinical data during the ICU stay and generates a complete, formatted discharge summary — ready for review in under 2 minutes.
The Role of AI in Modern ICU Documentation
The documentation burden in intensive care is well-established. Studies consistently show that ICU physicians spend 30–40% of their working time on documentation — time taken directly from patient care, teaching, and clinical decision-making.
Artificial intelligence, specifically large language models, offers a practical solution: generating draft discharge summaries from structured clinical data collected during the ICU stay.
How AI-Assisted Documentation Works
The approach is straightforward:
- During the ICU stay: Clinicians enter structured daily notes — vitals, medications, procedures, lab values, severity scores, clinical assessments. This takes 3–5 minutes per day as part of routine ward rounds.
- At discharge: The AI reads the complete set of structured daily entries and generates a coherent, comprehensive discharge summary.
- Physician review: The clinician reviews the generated summary, makes any necessary corrections or additions, and signs off.
The result is a complete draft in minutes rather than hours — and because it is generated from structured data entered throughout the stay, it is typically more complete than a summary written from memory at discharge.
For a deep dive into how AI is changing ICU documentation workflows, see our article on AI-powered ICU discharge documentation.
What AI Does Well
- Synthesis of large datasets: Consolidating 14 days of daily notes, lab values, and medication changes into a coherent narrative
- Completeness: Structured input ensures that all required sections are populated — no forgotten components
- Consistency: Every summary follows the same structure, with the same level of detail
- Speed: Draft generation in under 2 minutes for even the most complex ICU stays
What AI Cannot Replace
- Clinical judgement: The AI does not decide what is clinically significant — the physician does, through what they choose to document in daily notes
- Nuanced interpretation: Complex clinical reasoning, differential diagnosis discussions, and prognostic assessments require human expertise
- Accountability: The physician remains the author and the responsible party — AI is a drafting tool, not a replacement
AI-generated summaries are drafts, not final documents. The reviewing physician must verify accuracy, add clinical reasoning where needed, and take responsibility for the final content. The AI accelerates the mechanical work of documentation; the clinical thinking remains entirely human.
The Structured Data Advantage
The quality of an AI-generated discharge summary depends entirely on the quality of the input data. This is why the structured daily note approach is critical: if vitals, medications, procedures, and severity scores are entered systematically each day, the AI has a complete dataset to work with.
Contrast this with an AI that attempts to generate a summary from unstructured, handwritten notes or fragmented EMR entries — the output will reflect the gaps and inconsistencies in the input.
ICU Discharge Summaries for Special Populations
Patients Who Die in the ICU
When a patient dies during the ICU stay, the discharge summary becomes a death summary — a document with additional requirements including cause-of-death chain documentation, family counselling records, and circumstances of death. For a comprehensive guide, see How to Write an ICU Death Summary.
Long-Stay ICU Patients (>14 Days)
For patients with prolonged ICU stays, the phase-based approach to the clinical course becomes essential. Organise by clinical phases (e.g., “Septic shock and resuscitation,” “Ventilator-dependent phase,” “Weaning and rehabilitation”) rather than attempting a day-by-day account.
Consider including an interim summary at the 7-day or 14-day mark for patients with ongoing ICU stays. This reduces the documentation burden at final discharge and creates a contemporaneous record while events are still fresh.
Patients Transferred to Another Facility
Inter-facility transfers require additional documentation:
- Reason for transfer (higher level of care, specialist services, patient/family preference)
- Clinical condition at time of transfer, including ventilator settings and infusion rates
- Specific handoff information for the receiving team
- Contact details for the transferring intensivist
ICU Discharge Summary Template
For reference, here is a template structure that covers all essential components:
| Section | Contents |
|---|---|
| Patient Demographics | Name, age, sex, MRN, admission/discharge dates |
| Admission Details | Source, admitting diagnosis, indication for ICU, comorbidities, baseline function |
| Severity Scores | SOFA (with components), APACHE II, GCS at admission |
| Clinical Course | Phase-by-phase narrative of the ICU stay |
| Procedures | Each procedure with date, indication, operator, outcome |
| Medications | Vasopressors, antibiotics, sedation, anticoagulation, discharge medications |
| Investigations | Key lab trends, culture results, imaging findings |
| Complications | Each complication with detection and management |
| Family Communication | Prognosis discussions, goals of care, consent |
| Discharge Condition | Vitals, consciousness, respiratory status, functional status |
| Discharge Plan | Medications, follow-up, pending results, red flags |
| Author and Attestation | Writing physician, supervising intensivist, date/time |
Print or bookmark this template and use it as a checklist every time you write a discharge summary. Even experienced intensivists benefit from a systematic prompt — it is easier to confirm “this section is not applicable” than to remember every section from scratch.
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Conclusion
The ICU discharge summary is a document that serves clinical, legal, financial, and quality purposes simultaneously. Writing one well requires systematic data collection during the ICU stay, a structured approach to synthesis at discharge, and attention to the specific requirements of each section.
The key principles are consistent across institutions and countries: be complete, be accurate, show your clinical reasoning, and make the follow-up plan actionable. Severity scores like SOFA and APACHE II should be documented with component-level detail. Complications should be documented factually, not defensively. And the clinical course should tell a coherent story — not repeat daily notes verbatim.
For patients who die during the ICU stay, additional requirements apply — see our complete guide to ICU death summaries. For insurance-specific documentation, see the guide on ICU discharge summaries for TPA insurance claims. And for clinicians looking to reduce documentation time without sacrificing quality, explore how AI is transforming ICU discharge documentation.
Tools like Rivara Health’s ICU Summary Generator are built to address the documentation burden directly — collecting structured data during the stay and generating the complete discharge summary at the end. The clinical thinking is yours; the mechanical work of assembly is automated.
Related reading:
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Reduce ICU Documentation Time by 90%
Generate medicolegal-grade ICU discharge summaries in under 2 minutes. Built for Indian hospitals, designed for TPA compliance.