Medicolegal documentation in the ICU is the single most important factor that determines the outcome of clinical negligence claims involving critically ill patients. Across every jurisdiction — from the United States to India, the United Kingdom to Australia — courts consistently hold that the clinical record is the primary evidence of what care was provided, when, and why. When documentation is absent, incomplete, or contradictory, the legal presumption shifts against the treating clinician regardless of the actual quality of care delivered.
Intensive care units present unique documentation challenges. Patients are frequently incapacitated, decisions are made under extreme time pressure, multiple specialists contribute to management simultaneously, and the risk of adverse outcomes is inherently high. These conditions create an environment where documentation failures are both more likely to occur and more consequential when they do.
This guide provides a global framework for medicolegal ICU documentation — drawing on legal principles and professional standards from multiple jurisdictions — to help intensivists build clinical records that are defensible, auditable, and compliant with international governance expectations.

What Is Medicolegal Documentation and Why It Matters in ICU
Medicolegal documentation refers to the creation and maintenance of clinical records that serve both a medical purpose (guiding patient care) and a legal purpose (providing admissible evidence of the care provided). In the ICU context, every clinical note, order, consent form, and nursing observation becomes a potential legal document.
The stakes are higher in intensive care than in almost any other clinical setting:
- Mortality is expected. ICU mortality rates range from 10% to 40% depending on case mix and geography. Every death is a potential trigger for litigation.
- Decisions are high-risk. Intubation, vasopressors, renal replacement therapy, and invasive procedures all carry significant complication rates.
- Patients cannot advocate for themselves. Most ICU patients are sedated, intubated, or otherwise incapacitated — they cannot later testify about the care they received.
- Multiple clinicians are involved. Shared care among intensivists, surgeons, and subspecialists creates documentation gaps and conflicting records.
The fundamental principle of medicolegal documentation is simple: if it isn’t documented, it didn’t happen. This legal maxim — recognised across common law and civil law jurisdictions alike — means that a doctor who provided excellent care but documented poorly is in a weaker legal position than a doctor who provided average care but documented meticulously.
The Documentation Paradox in Critical Care
ICU clinicians face a genuine paradox. The moments when documentation matters most — resuscitation, acute deterioration, emergency procedures — are precisely the moments when there is least time to document. Yet courts and regulators evaluate clinical conduct primarily through the written record, not through testimony about what the clinician remembers happening.
Resolving this paradox requires systems-level solutions: structured templates, real-time data capture, standardised severity scoring, and digital tools that reduce the documentation burden without sacrificing medicolegal rigour.
Legal Principles Governing ICU Documentation
While specific laws vary by jurisdiction, several core legal principles apply universally to ICU documentation.
Duty of Care and Standard of Care
Every clinician who treats a patient in the ICU owes a duty of care — the legal obligation to provide treatment that meets the accepted standard. The standard of care is defined as what a reasonably competent clinician of the same specialty would have done in similar circumstances.
In negligence litigation, the central question is whether the clinician’s conduct fell below this standard. The clinical record is the primary evidence used to answer that question.
The standard of care is not perfection — it is reasonableness. Courts do not expect zero complications or zero deaths. They expect that the clinician identified the problem, considered the options, made a defensible decision, and acted on it in a timely manner. The documentation must show this chain of reasoning.
The Duty to Document
Beyond the duty to provide care, clinicians have a distinct duty to document that care. Professional regulatory bodies worldwide — including the General Medical Council (UK), the American Medical Association (US), the Medical Council of India, and the Australian Health Practitioner Regulation Agency — require physicians to maintain accurate, contemporaneous clinical records.
Failure to document is itself a breach of professional duty, independent of whether the clinical care was adequate.
Informed Consent as a Legal Requirement
Informed consent is both an ethical principle and a legal requirement in every major jurisdiction. In the ICU, where patients are often unable to consent personally, the law requires:
- That consent is obtained from an authorised surrogate decision-maker
- That the consent covers the specific procedure, its risks, benefits, and alternatives
- That the consent discussion is documented in the clinical record
The legal standard for informed consent has evolved significantly. The old Bolam standard (what a reasonable doctor would disclose) has been replaced in many jurisdictions by the Montgomery standard (what a reasonable patient would want to know). This shift places greater emphasis on documenting the specific risks discussed and the patient or surrogate’s understanding of those risks.
Burden of Proof and the Evidentiary Role of Records
In most civil negligence claims, the burden of proof lies with the plaintiff (the patient or family). However, when clinical records are missing, incomplete, or contradictory, courts routinely apply an adverse inference — presuming that the missing documentation would have been unfavourable to the defendant.
This means that gaps in ICU documentation do not simply leave questions unanswered — they actively create legal liability.
Courts in the UK, US, India, and Australia have all applied adverse inferences to missing medical records. An incomplete ICU chart is not neutral — it is presumed unfavourable. Every gap is a vulnerability.
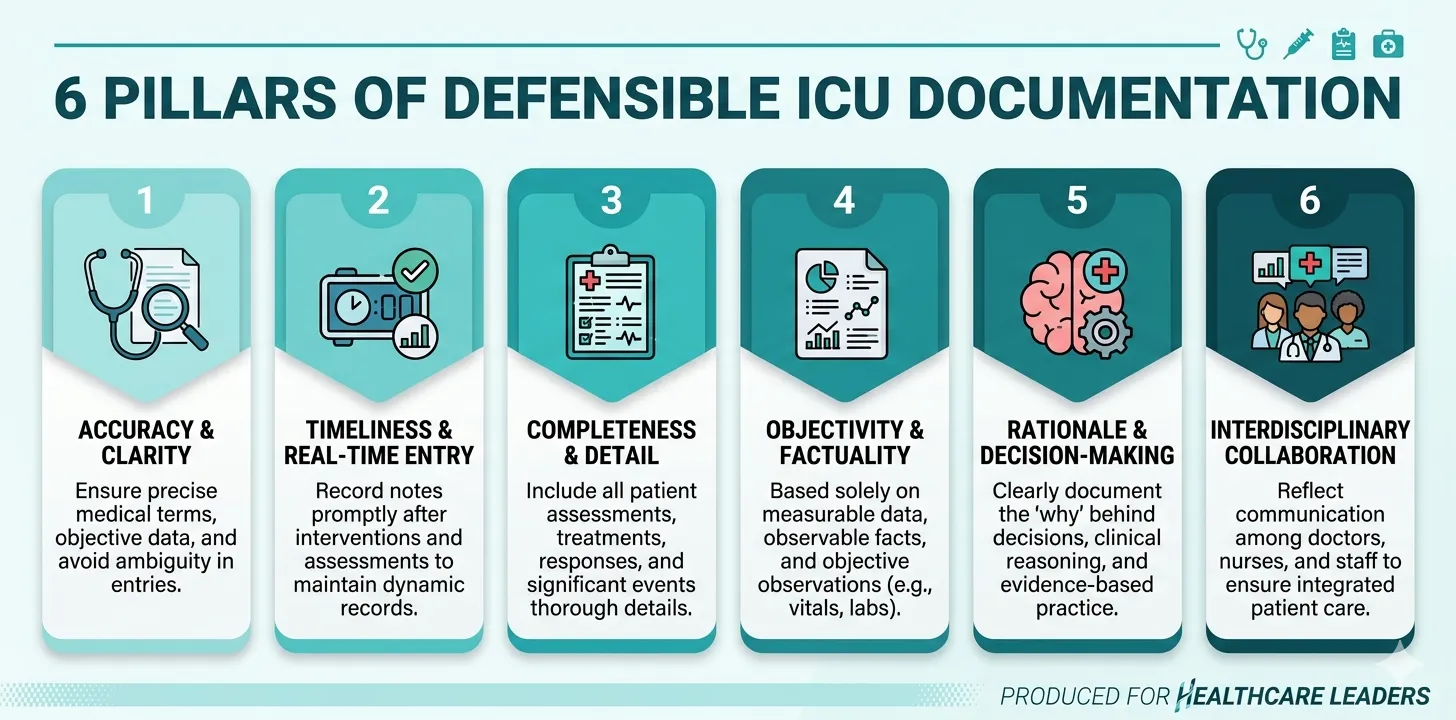
Essential Elements of Defensible ICU Records
A medicolegally defensible ICU record has six core characteristics. Every entry, from admission to discharge or death, must embody these principles.
1. Contemporaneous Documentation
Document at the time of the event or as close to it as possible. Notes written hours or days after the event carry significantly less evidentiary weight and may be viewed with suspicion — particularly if they follow a complication or adverse outcome.
Practical standard: Clinical notes should be entered during or immediately after ward rounds. Significant events (cardiac arrest, acute deterioration, emergency procedures) should be documented as soon as the situation is stabilised.
2. Clinical Reasoning — Not Just Actions
The most protective element of medicolegal documentation is documented clinical reasoning. Courts do not just ask what you did — they ask why you did it, what alternatives you considered, and what evidence supported your decision.
“Blood cultures returned ESBL-producing E. coli, resistant to cephalosporins. Changed from ceftriaxone to meropenem 1g 8-hourly based on sensitivity pattern. Discussed with microbiology (Dr. Chen). Patient’s renal function stable (creatinine 1.2 mg/dL); no dose adjustment required.”
This note demonstrates culture-guided prescribing, specialist input, awareness of renal dosing, and a systematic approach — making negligence nearly impossible to establish.
Apply the “lawyer’s question” test to every significant clinical decision: if a lawyer could ask “Doctor, why did you do that?”, then both the action and the reasoning must be in the record.
3. Objective, Specific Language
Medicolegal documentation must use precise, measurable language — not subjective assessments.
| Avoid | Use Instead |
|---|---|
| ”Patient not doing well" | "MAP declined from 70 to 52 mmHg over 3 hours despite norepinephrine 0.2 mcg/kg/min" |
| "Condition worsening" | "SOFA score increased from 8 to 14 over 48 hours; new renal and hepatic dysfunction" |
| "Family counselled" | "Spoke with patient’s wife (Mrs. Torres) at 14:00. Explained worsening multi-organ dysfunction and high mortality risk. Family expressed understanding." |
| "Consent taken" | "Risks of tracheostomy (bleeding, infection, tracheal stenosis, failure) explained to patient’s son. Written consent obtained.” |
4. Completeness Over Brevity
The medicolegal standard for documentation is higher than the clinical standard. What is clinically obvious must still be documented if it could become a point of dispute.
Document:
- Every significant clinical decision and the reasoning behind it
- Every procedure with indication, technique, and outcome
- Every medication change with rationale
- Every communication with family or surrogate decision-makers
- Every instance of clinical deterioration or improvement
- Every deviation from a standard protocol, with justification
- Negative findings that are clinically relevant (e.g., “No pneumothorax on post-procedure CXR”)
5. Accurate Identification and Attribution
Every clinical entry must include:
- Date and time (24-hour clock)
- Author (name, designation, and role)
- Patient identifiers (name, hospital number)
- Signature (physical or electronic)
In shared-care environments like the ICU, it must be clear who wrote each note and in what capacity. Notes by junior trainees, nursing staff, and consultants should be clearly distinguishable.
6. Immutability and Audit Trails
Clinical records must not be altered after the fact. If an error needs correction, the original entry must remain visible, with the correction appended as a new, dated entry. This principle — fundamental to both paper and electronic records — ensures the integrity of the clinical record as evidence.
Record integrity is not just a best practice — it is a legal requirement. Altered medical records can constitute spoliation of evidence, carrying sanctions ranging from adverse inferences to criminal charges depending on the jurisdiction. An append-only record design eliminates this risk entirely.
Informed Consent in ICU: Challenges and Best Practices
Informed consent in the ICU is fundamentally different from elective settings. The challenges are both clinical and legal.
The Incapacitated Patient Problem
The majority of ICU patients cannot provide personal consent due to sedation, intubation, altered consciousness, or cognitive impairment. This triggers the legal framework for surrogate decision-making, which varies by jurisdiction:
| Jurisdiction | Surrogate Framework | Key Statute |
|---|---|---|
| United States | Healthcare proxy / durable power of attorney; absent these, state-defined next-of-kin hierarchy | Varies by state; Uniform Health-Care Decisions Act |
| United Kingdom | Best interests assessment under the Mental Capacity Act; lasting power of attorney | Mental Capacity Act 2005 |
| India | Next of kin consent; no formal advance directive legislation until Mental Healthcare Act 2017 | Consumer Protection Act 2019; MHA 2017 |
| European Union | Varies by member state; advance directives recognised in most jurisdictions | Oviedo Convention (Council of Europe) |
| Australia | Substitute decision-maker hierarchy; enduring power of attorney | Varies by state/territory |
Emergency Exception
All jurisdictions recognise an emergency exception to informed consent — sometimes called the doctrine of necessity. When a patient is in immediate danger and no surrogate is available, the clinician may proceed with life-saving treatment without consent.
However, the emergency exception must be documented explicitly:
“Patient presented in haemorrhagic shock (MAP 40 mmHg, Hb 5.2 g/dL). No next of kin contactable. Emergency laparotomy performed under doctrine of necessity — delay for consent would have resulted in death. Next of kin (wife, Mrs. Nakamura) contacted at 03:45 and informed of surgery.”
The emergency exception does not mean consent documentation is unnecessary — it means the documentation must explain why consent could not be obtained and why the intervention was immediately necessary. An undocumented emergency procedure is legally indistinguishable from a procedure performed without consent.
Documenting Consent Properly
A consent note must include:
- Who consented — the patient (if competent) or the surrogate (with name, relationship, and legal authority)
- What was explained — diagnosis, proposed intervention, material risks, expected benefits, and alternatives (including no intervention)
- Specific risks discussed — particularly for high-risk ICU procedures (tracheostomy, central line insertion, renal replacement therapy)
- Confirmation of understanding — that the consenting party understood the information and had the opportunity to ask questions
- The clinician who obtained consent — name and designation
“Informed consent obtained” is not adequate documentation. The note must specify what risks were communicated and who consented. A signed consent form without a corresponding clinical note explaining the discussion is weak evidence of genuine informed consent.
Structured ICU documentation — built for medicolegal defensibility
Rivara Health captures timestamped, append-only clinical data including consent records, clinical reasoning, and family interactions — creating the audit trail that medicolegal experts recommend.
Audit Trails and Record Integrity
An audit trail is a chronological record of every action taken on a clinical document — who created it, when, and any subsequent modifications. In medicolegal proceedings, the integrity of the audit trail can be as important as the clinical content of the record.
The Who-What-When Framework
Every entry in an ICU clinical record must answer three questions:
- Who made the entry? (Name, role, designation)
- What was documented? (Clinical observation, decision, procedure, communication)
- When was the entry made? (Date, time — ideally system-generated, not manually entered)
Append-Only Design
The gold standard for medicolegal record integrity is an append-only system where entries cannot be modified or deleted after submission. New information is added as subsequent entries, and corrections are made by appending a correction note that references the original entry.
This design mirrors the legal standard for admissible evidence and eliminates allegations of record tampering — a claim that can be devastating in litigation regardless of its merit.
Electronic vs Paper Audit Trails
Paper records rely on handwriting analysis, ink consistency, and physical integrity to demonstrate authenticity. Electronic records rely on system-generated timestamps, user authentication logs, and version histories.
Courts increasingly favour electronic records precisely because their audit trails are more robust and harder to manipulate. However, electronic systems must be properly configured — a system that allows back-dating or silent editing of records may be worse than paper from a medicolegal perspective.
When evaluating or implementing an electronic documentation system for the ICU, the two non-negotiable medicolegal features are: (1) system-generated timestamps that cannot be overridden by users, and (2) append-only design where previous entries remain permanently visible even after corrections.
Common Documentation Failures That Lead to Legal Liability
Analysis of medical malpractice claims across jurisdictions reveals consistent patterns of documentation failure. Understanding these patterns allows clinicians to proactively address the most dangerous gaps.
1. Missing or Delayed Resuscitation Records
CPR documentation is one of the most legally scrutinised elements of ICU records. Incomplete or absent CPR records — particularly the timeline of events and drugs administered — are a frequent basis for negligence claims.
Required CPR documentation (Utstein template):
- Time of arrest recognition
- Initial cardiac rhythm
- Time CPR commenced
- All drugs administered with doses and times
- Defibrillation attempts with energy levels
- Response to interventions (ROSC achieved or not)
- Time of death pronouncement (if unsuccessful)
- Personnel present
2. Absent Family Communication Records
The most common allegation in ICU negligence claims globally is: “We were never told how serious it was.” If family counselling is not documented, courts presume it did not occur.
Best practice: Document every family interaction — including informal bedside conversations — with the date, time, attendees, content discussed, and the family’s expressed understanding.
3. Undocumented Deviations from Protocol
When a clinician deviates from a standard protocol or guideline, the deviation itself is not negligence — but the failure to document the reason for deviation can be. A documented deviation with clinical reasoning is defensible; an undocumented deviation invites the inference that it was an error.
4. Retrospective Documentation
Notes written long after the events they describe carry less evidentiary weight. Notes written after a complaint or adverse event is identified carry almost no weight and may be viewed as fabrication.
A post-hoc note entered after a complication or complaint has been flagged is worse than no note at all. It suggests awareness that the existing record was inadequate — and an attempt to fill the gap retrospectively. Contemporaneous documentation is the only defensible standard.
5. Inconsistencies Between Records
When the doctor’s notes, nursing notes, medication charts, and monitoring data tell different stories, the credibility of the entire record collapses. In shared-care environments like the ICU, inconsistencies are common and dangerous.
Example: If the nursing observation chart shows a MAP of 45 mmHg at 02:00 but the doctor’s note at 08:00 states “haemodynamically stable overnight,” a plaintiff’s lawyer will use this inconsistency to undermine the entire defence.
6. Severity Scores Not Documented
Objective illness severity scores — particularly SOFA scores and APACHE II — provide standardised, reproducible documentation of how sick a patient was. Without them, the clinician’s retrospective claim that “the patient was extremely ill” lacks evidentiary support.
| Documentation Failure | Legal Risk | Mitigation |
|---|---|---|
| Missing CPR records | Presumption of delayed or inadequate resuscitation | Use Utstein template for every arrest |
| No family communication log | ”We were never told” allegation | Document every interaction with time/attendees |
| Undocumented protocol deviation | Inference of error rather than clinical judgment | Always document reasoning for deviations |
| Retrospective notes | Viewed as fabrication; minimal evidentiary weight | Document during or immediately after events |
| Inconsistent multi-disciplinary records | Undermines credibility of entire chart | Regular record reconciliation; structured templates |
| No severity scoring | Cannot objectively demonstrate illness severity | Daily SOFA scores; admission APACHE II |
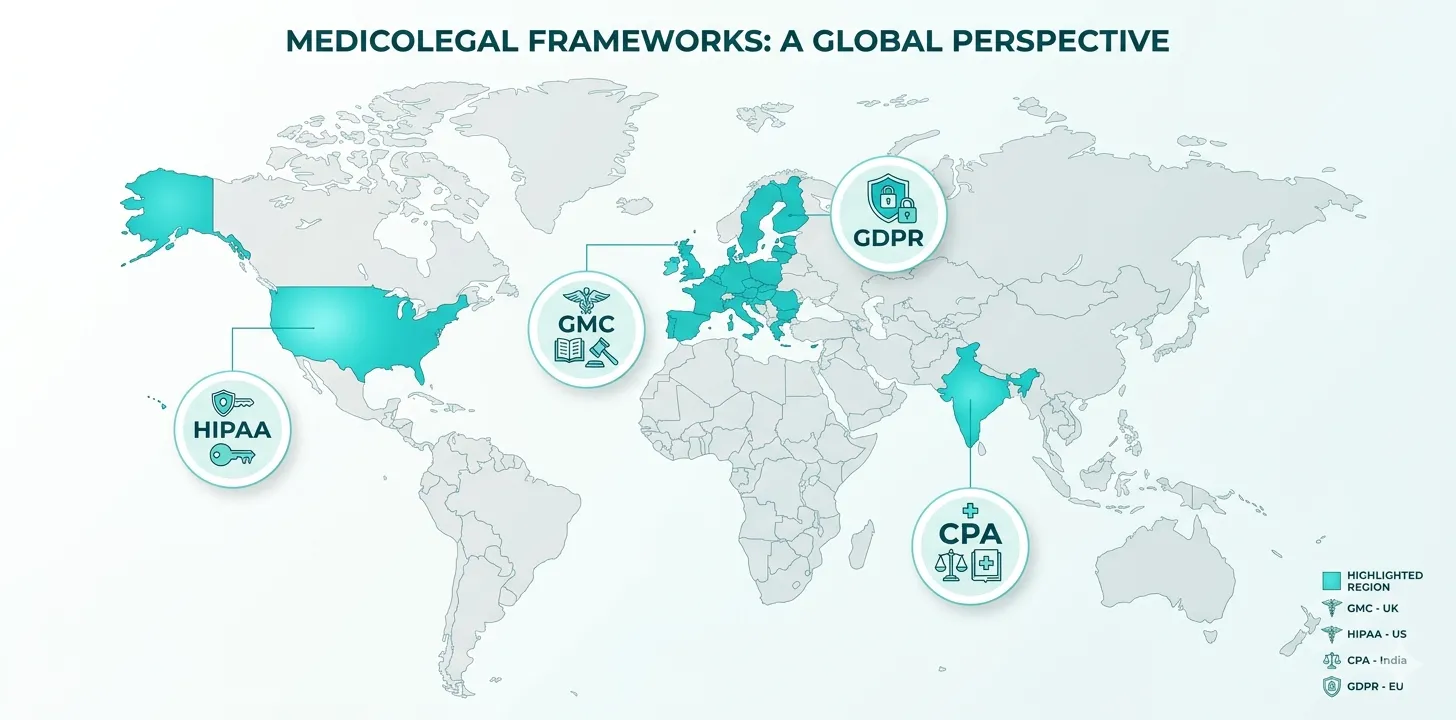
International Medicolegal Frameworks
While the core principles of defensible documentation are universal, clinicians must also understand the jurisdiction-specific requirements that apply to their practice.
United States: HIPAA and Malpractice Law
In the US, ICU documentation is governed by a combination of federal regulations (HIPAA for privacy and security), state malpractice statutes, and the Joint Commission (JCAHO) standards for accredited hospitals.
Key requirements:
- Medical records must be maintained for a minimum retention period (varies by state; typically 6–10 years for adults, longer for minors)
- HIPAA requires administrative, physical, and technical safeguards for electronic health records
- The standard of care in malpractice is defined by expert testimony — the clinical record is the primary evidence against which expert opinion is applied
- Tort reform legislation in many states caps non-economic damages but does not affect the evidentiary standard for documentation
United Kingdom: NHS Governance and GMC Standards
The UK operates under a comprehensive clinical governance framework, with medicolegal documentation standards set by the General Medical Council (GMC), NHS Resolution (for negligence claims), and the Medical Defence Organisations (MDU, MPS, MDDUS).
Key requirements:
- GMC’s Good Medical Practice requires doctors to “keep clear, accurate, and legible records” including “relevant clinical findings, decisions made, information given to patients, and any drugs or other treatment prescribed”
- NHS Resolution (formerly NHSLA) encourages a “duty of candour” — open disclosure of adverse events, which must be documented
- Medical records must be retained for 8 years (adults) or until the patient’s 25th birthday (minors)
- The Montgomery standard for informed consent requires documentation of all material risks
India: Consumer Protection Act and Medical Council Standards
In India, medical negligence claims are primarily adjudicated under the Consumer Protection Act, 2019 (CPA), with criminal negligence addressed under the Bharatiya Nyaya Sanhita. The Medical Council of India (now National Medical Commission) sets documentation standards.
Key requirements:
- Medical services are treated as “services” under the CPA, enabling consumer court jurisdiction
- Courts follow the Bolam test (via Jacob Mathew v State of Punjab, 2005) — the clinical record must demonstrate adherence to accepted medical practice
- Electronic records are admissible under the Bharatiya Sakshya Adhiniyam, 2023, with demonstrable audit trails
- For jurisdiction-specific guidance, see our detailed guide on medicolegal documentation in Indian ICUs
European Union: GDPR and Patient Rights
EU member states have additional requirements under the General Data Protection Regulation (GDPR), which classifies health data as a “special category” with heightened protection requirements.
Key requirements:
- Health data processing requires explicit legal basis (typically “necessary for medical treatment” or explicit consent)
- Patients have a right to access their medical records and request rectification of inaccurate data
- Data controllers (hospitals) must implement “privacy by design” in clinical documentation systems
- Record retention periods vary by member state but must be defined and justified
- Cross-border patient data transfers require specific safeguards
Despite jurisdictional differences, the global trend is clear: documentation standards are converging toward greater transparency, patient access, data integrity, and clinician accountability. An ICU record that meets the highest standard — contemporaneous, reasoned, complete, and immutable — will satisfy requirements in virtually any jurisdiction.
Digital Documentation vs Paper Records: Legal Standing
The transition from paper to electronic clinical records has significant medicolegal implications.
Admissibility of Electronic Records
Electronic health records (EHRs) are admissible as evidence in all major jurisdictions, provided they meet specific authentication requirements:
| Criterion | Paper Records | Electronic Records |
|---|---|---|
| Authentication | Handwriting analysis; witness testimony | System login credentials; digital signatures |
| Integrity | Physical examination for alterations | Audit trail; version history; hash verification |
| Contemporaneity | Ink dating (forensic); relative sequencing | System-generated timestamps |
| Attribution | Handwriting identification | User authentication logs |
| Completeness | Physical page integrity | Database integrity checks; backup verification |
Advantages of Electronic Documentation for Medicolegal Purposes
- Automatic timestamping eliminates disputes about when entries were made
- User authentication provides definitive attribution of every entry
- Append-only architecture prevents undetectable alterations
- Structured data capture ensures completeness (mandatory fields, auto-populated severity scores)
- Searchability allows rapid retrieval for legal review
- Backup and redundancy protect against record loss
Risks of Poorly Implemented Electronic Systems
Not all electronic systems enhance medicolegal protection. Systems that allow:
- Backdating of entries
- Silent editing without audit trails
- Overwriting of previous values
- Copy-paste propagation of outdated information
…may create greater legal vulnerability than paper records, because they give a false impression of integrity while lacking it.
Copy-paste — also called “cloned documentation” — is one of the most dangerous practices in electronic ICU records. Carrying forward yesterday’s assessment without updating it creates a record that appears complete but may be clinically inaccurate. Courts have successfully used copy-paste evidence to demonstrate that clinicians were not genuinely assessing patients.
How AI Tools Support Medicolegal Documentation
Artificial intelligence is emerging as a powerful tool for improving the quality and consistency of ICU documentation without adding to the clinician’s workload.
Structured Data Synthesis
AI tools can synthesise structured daily ICU data — vitals, ventilator parameters, medications, laboratory results, SOFA scores — into coherent clinical narratives. This ensures that the complete clinical picture is captured in the record, even when clinicians are pressed for time.
The resulting documentation maintains the completeness and objectivity standards required for medicolegal defensibility, while reducing the time clinicians spend writing narrative notes.
Automated Severity Scoring
Accurate severity scoring at admission and throughout the ICU stay — APACHE II, SOFA, and others — provides objective, standardised documentation of illness severity. AI tools that automatically calculate and track these scores eliminate both the calculation errors and the documentation gaps that occur when scoring is done manually.
This is particularly valuable in medicolegal contexts where the clinical trajectory must be demonstrated objectively. A chart showing daily SOFA scores rising from 6 to 18 tells a more defensible story than a narrative note stating “patient continued to deteriorate.”
Consistent Discharge and Death Summary Generation
AI-generated summaries that draw on structured daily data ensure that discharge and death summaries are comprehensive and internally consistent. Every procedure, medication change, family interaction, and clinical decision recorded during the stay is reflected in the final document — eliminating the gaps that occur when summaries are written from memory.
AI-generated documentation does not replace clinical judgment — it augments the clinician’s ability to create a complete, consistent record. The clinician reviews, validates, and approves every AI-generated note before it becomes part of the permanent record. This combination of AI completeness and human oversight represents the current best practice for medicolegal documentation.
For a deeper exploration of how AI is transforming ICU documentation workflows, see our guide on AI in ICU discharge documentation.
AI-powered documentation that meets medicolegal standards
Rivara Health's ICU Summary Generator captures structured clinical data, auto-calculates severity scores, and generates comprehensive summaries — all with timestamped, append-only audit trails.
A Medicolegal Documentation Checklist for ICU Clinicians
Use this checklist to evaluate whether your ICU documentation meets the medicolegal standard:
At Admission
- Complete admission note with history, examination, and working diagnosis
- Severity score documented (APACHE II and/or SOFA)
- Comorbidities listed with current treatments
- Informed consent documented for initial procedures (or emergency exception noted)
- Initial family counselling documented with attendees and content
- Admission time recorded precisely (not just date)
Daily Documentation
- Contemporaneous ward round note with current clinical assessment
- Updated SOFA score or other severity metric
- All medication changes with rationale
- Ventilator parameters and any changes in respiratory management
- Vasopressor doses and haemodynamic targets
- Fluid balance
- New investigation results and their interpretation
- Clinical reasoning for management decisions
- Family communication (if any occurred)
At Critical Events
- Time of event documented precisely
- Clinical presentation at the time of the event
- Immediate management documented chronologically
- Personnel present
- Family notified (when and by whom)
- Outcome of the event
At Discharge or Death
- Comprehensive summary covering the entire clinical course
- Cause-of-death chain (for deaths) in WHO format
- All family counselling sessions referenced
- All procedures listed with dates and outcomes
- Condition at discharge or circumstances of death
- Follow-up plan or post-mortem documentation
- TPA/insurance documentation complete (where applicable)
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Conclusion
Medicolegal documentation in the ICU is not a bureaucratic burden separate from clinical care — it is an integral component of clinical care itself. The clinical record is simultaneously a care coordination tool, a communication document, a quality assurance record, and a legal instrument. When documentation is thorough, contemporaneous, and reasoned, it protects clinicians in litigation, supports insurance claims for patients’ families, and contributes to clinical governance and quality improvement.
The principles are universal: document what you observed, what you decided, why you decided it, what you did, and what you communicated — in real time, using objective language, with clear attribution. Whether you practise in New York, London, Mumbai, or Berlin, these principles will produce a record that satisfies both clinical and legal scrutiny.
For ICU teams looking to strengthen their documentation practice without adding workload, structured digital tools offer the most practical path forward. Rivara Health’s ICU Summary Generator combines real-time data capture, automated severity scoring, and AI-powered summary generation with the append-only, timestamped audit trail design that medicolegal standards demand.
Related reading: How to Write an ICU Death Summary | ICU Discharge Summaries: A Complete Guide | SOFA Score in ICU: Complete Guide for Clinicians | How AI Is Transforming ICU Discharge Documentation | ICU TPA Insurance Documentation
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Reduce ICU Documentation Time by 90%
Generate medicolegal-grade ICU discharge summaries in under 2 minutes. Built for Indian hospitals, designed for TPA compliance.