Medical negligence cases against ICU doctors in India have risen sharply over the past decade. The National Consumer Disputes Redressal Commission (NCDRC) and state consumer forums regularly hear cases involving ICU deaths, delayed interventions, and alleged failures in communication. In the majority of these cases, the outcome hinges not on the quality of care provided, but on the quality of documentation.
A doctor who provided excellent care but documented poorly is in a weaker legal position than a doctor who provided average care but documented meticulously. This is the uncomfortable reality of medicolegal practice in Indian ICUs.
This guide covers the core principles of medicolegal documentation in ICU practice, the legal framework governing medical negligence in India, and specific documentation strategies that protect doctors without adding unreasonable burden to their workflow.
The Legal Framework: Medical Negligence in India
Consumer Protection Act, 2019
Medical services fall under the Consumer Protection Act (CPA), 2019, which replaced the earlier 1986 Act. Under the CPA:
- Medical services are treated as services under the Act
- Patients (or their families) can file complaints alleging deficiency in service
- The burden of proof lies on the complainant, but if the medical record is incomplete, the presumption shifts against the doctor
- Consumer courts can award compensation for negligence, including emotional distress
The Standard for Medical Negligence
Indian courts follow the Bolam test (established in Bolam v Friern Hospital Management Committee, 1957, and adopted by the Indian Supreme Court in Jacob Mathew v State of Punjab, 2005):
A doctor is not negligent if they acted in accordance with a practice accepted as proper by a responsible body of medical opinion — even if other doctors would have acted differently.
The Bolam test protects doctors who follow accepted medical practice. But the key question in court is: how do you prove you followed accepted practice? The answer is always the same — through the clinical documentation. If the record shows that you followed a recognized protocol, you are protected. If the record is silent, you are vulnerable.
Criminal Medical Negligence
Under Section 304A of the Indian Penal Code (now Section 106 of the Bharatiya Nyaya Sanhita, 2023), death caused by a rash or negligent act is a criminal offence. The Supreme Court in Jacob Mathew clarified that criminal prosecution of doctors should only be for gross negligence — not ordinary negligence or error of judgment.
However, the distinction between “ordinary” and “gross” negligence often depends on the documentation. A well-documented clinical record that shows a systematic, considered approach to care makes it difficult to establish gross negligence — even if the outcome was unfavorable.
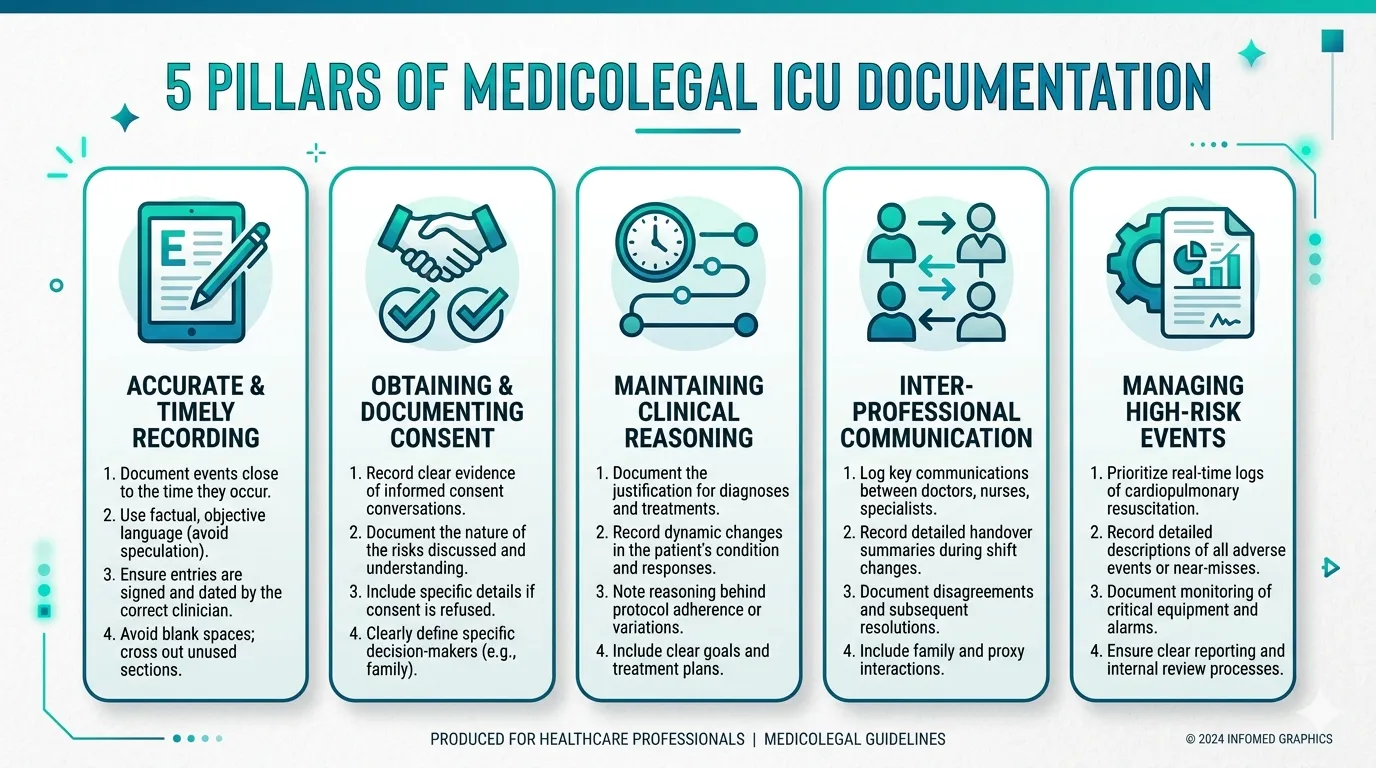
The Five Pillars of Medicolegal ICU Documentation
1. Contemporaneous Documentation
Document at the time of the event, not afterwards.
Retrospective documentation — writing notes hours or days after the event — is inherently less credible in legal proceedings. Courts give significantly more weight to contemporaneous records.
Notes written after a complication or death are viewed with suspicion. If a complication occurs at 14:00 and the note documenting it is timestamped 22:00, the court may question whether the note accurately reflects what happened — or whether it was constructed after the fact to justify the management.
Practical strategy: Enter daily ICU notes during or immediately after the ward round. If a significant event occurs (cardiac arrest, new complication, emergency procedure), document it as soon as the situation is stabilised — not at the end of the shift.
2. Completeness Over Brevity
Document everything clinically significant, even if it seems redundant.
The medicolegal standard for documentation is higher than the clinical standard. What is clinically obvious (e.g., “of course we checked potassium before giving succinylcholine”) must still be documented if it could become a point of dispute.
What to document:
- Every significant clinical decision and the reasoning behind it
- Every procedure, with indication and outcome
- Every change in medication, with rationale
- Every communication with the family
- Every instance where the patient’s condition changed
- Every deviation from a standard protocol, with the reason
A useful test: if a lawyer could ask “Doctor, why did you do X?” — then X should be documented in the clinical record, along with the answer to that question.
3. Objective, Factual Language
Document what you observed, measured, and did — not opinions or speculations.
Good medicolegal documentation uses:
- Specific vital signs, lab values, and clinical findings
- Timestamps
- Names of staff involved
- Exact drug doses and routes
- Objective descriptions of the patient’s condition
Avoid subjective or ambiguous language in clinical notes.
Avoid: “Patient not doing well.” “Condition worsening.” “Family difficult.”
Instead: “MAP declined from 72 to 55 mmHg between 08:00 and 10:00 despite norepinephrine 0.1 µg/kg/min. Dose increased to 0.15 µg/kg/min at 10:15.” “Family counselled at 11:00 regarding worsening haemodynamic status. Son (Mr. Rajesh Kumar) expressed concern about prognosis. Explained that the situation is critical with significant risk of mortality.”
4. Document Clinical Reasoning
Record not just what you did, but why you did it.
This is the single most protective element of medicolegal documentation. If a court can see that the doctor considered the clinical situation, weighed the options, and made a reasoned decision, negligence is extremely difficult to establish.
“Culture returned Acinetobacter baumannii, sensitive only to colistin and polymyxin B. After discussion with Infectious Disease team (Dr. Sharma), decision made to initiate IV colistin 9 MIU loading dose followed by 4.5 MIU 12-hourly. Patient’s renal function (creatinine 2.1 mg/dL) to be monitored closely given nephrotoxic potential. Alternative agent polymyxin B considered but not available in hospital pharmacy.”
This note is medicolegally bulletproof. It shows: (1) the culture-guided basis for the decision, (2) specialist consultation, (3) awareness of the drug’s side effects, (4) a plan to monitor for complications, and (5) why the alternative was not used. A lawyer would struggle to find negligence in this documentation.
5. Immutable, Tamper-Evident Records
Clinical records must not be altered after the fact.
Indian courts take a very dim view of altered medical records. Under Section 65B of the Indian Evidence Act (now Section 63 of the Bharatiya Sakshya Adhiniyam, 2023), electronic records are admissible as evidence — but their integrity must be demonstrable.
Handwritten notes that show signs of overwriting, deletion, or insertion will be scrutinised. Electronic records must have audit trails showing who entered what and when.
This is one of the strongest arguments for electronic clinical documentation with append-only design. A system where entries cannot be modified after saving — only new entries can be added — creates a tamper-evident record that mirrors the legal standard for admissible evidence.
Tamper-proof ICU documentation — built for medicolegal scrutiny
Every entry in Rivara Health's ICU Summary Generator is timestamped and append-only. No record can be altered after saving — creating an immutable clinical audit trail.
Specific Documentation Requirements by Scenario
Informed Consent
Informed consent in the ICU context is complex because patients are often incapacitated and decisions must be made urgently.
Document:
- Who consented (patient if competent, or next-of-kin with relationship specified)
- What was explained (diagnosis, proposed procedure, risks, benefits, alternatives)
- Whether the person understood and agreed
- Any specific risks that were highlighted (especially for high-risk procedures)
High-risk consent scenarios in ICU:
- Endotracheal intubation and mechanical ventilation
- Central venous catheter insertion
- Tracheostomy
- Renal replacement therapy (dialysis)
- High-risk medications (colistin, thrombolytics)
- Surgical procedures in critically ill patients
- Blood and blood product transfusion
“Informed consent taken” written in the notes without any detail about what was discussed is legally worthless. The consent must document what risks were communicated and acknowledged. A consent form signed by the family without a corresponding note explaining the discussion is weak evidence.
Against Medical Advice (AMA) / Leave Against Medical Advice (LAMA)
When a family requests discharge against medical advice from the ICU:
- Document who requested AMA and their relationship to the patient
- Document what you explained about the risks of leaving (including risk of death)
- Document that the family understood and still wished to proceed
- Obtain written LAMA documentation signed by the family member
- Document the patient’s clinical condition at the time of LAMA
- Document what medications/instructions were provided despite LAMA
If the family refuses to sign the LAMA form, document this refusal in the clinical notes: “Family (Mr. Suresh Kumar, son) requested removal of ventilatory support and discharge against medical advice. Explained that discontinuation of ventilatory support in patient’s current condition (GCS 6, FiO₂ 0.8, vasopressor-dependent) carries near-certain risk of death. Family acknowledged this risk verbally but declined to sign LAMA documentation. Witnessed by Nurse [Name] and Dr. [Name].”
Cardiopulmonary Resuscitation (CPR)
CPR documentation must follow a structured format:
- Time of arrest (when it was discovered, not when CPR was started)
- Initial rhythm (asystole, PEA, VF, VT)
- Time CPR was initiated
- Interventions: Chest compressions, defibrillation (number of shocks, joules), drugs administered (with doses and timing — e.g., “Adrenaline 1mg IV at 03:50, 03:53, 03:56”)
- Response to interventions (ROSC achieved? If so, when? If not, duration of resuscitation)
- Time of death pronouncement (if unsuccessful)
- Who was present during the resuscitation
- Whether the family was informed and their response
Complications and Adverse Events
When a complication occurs, document:
- What happened (specific clinical event)
- When it was identified (time)
- What was done (immediate management)
- Whether it was a recognised complication of the underlying condition or a procedure
- Whether the family was informed
Never avoid documenting a complication because you fear it will be used against you. The opposite is true: a documented complication that was promptly identified and appropriately managed is evidence of good care. An undocumented complication that is later discovered (through lab reports, radiology, or post-mortem) is evidence of a cover-up.
What Consumer Courts Look For
Based on reported NCDRC and state consumer commission cases involving ICU care, courts typically examine:
-
Was the patient’s condition assessed and documented at admission? (History, examination, investigations, severity scoring)
-
Were appropriate investigations and treatments initiated in a timely manner? (Documented with timestamps)
-
Was the patient monitored adequately? (Regular clinical notes, vitals, daily assessment)
-
Were complications identified and managed promptly? (Time of identification, management, outcome)
-
Was the family informed of the patient’s condition, prognosis, and significant events? (Documented counselling sessions)
-
Was informed consent obtained for procedures? (Documented consent with risks explained)
-
Were specialist consultations sought when appropriate? (Documented with specialist’s name, opinion, and plan)
-
Does the clinical record support the clinical decisions made? (Documentation of reasoning, not just actions)
Consumer courts do not expect perfection. They expect reasonable care, provided systematically, with adequate documentation. The doctor who documents a complication that arose despite appropriate care is in a far stronger position than the doctor who provided the same care but didn’t document it.
Structured documentation that stands up in court
Rivara Health captures timestamped, append-only clinical data throughout the ICU stay — creating the kind of audit trail that medicolegal experts recommend.
7 Practical Strategies for Busy ICU Doctors
-
Use structured templates. Structured daily notes ensure you don’t forget critical elements. A template that prompts for vitals, ventilator settings, vasopressor doses, GCS, fluid balance, medications, and clinical assessment is far more reliable than free-text notes.
-
Document decisions, not just actions. “Started meropenem” is a clinical action. “Started meropenem empirically for suspected hospital-acquired pneumonia, pending BAL culture — covers likely Gram-negative pathogens per hospital antibiogram” is a documented decision. The second version is medicolegally defensible.
-
Timestamp every note. Get into the habit of starting every note with the date and time. In handwritten records, this is often missing. In electronic records, it should be automatic.
-
Document family interactions every time. Even brief conversations. “Spoke with patient’s wife at bedside during evening round. Explained current clinical status and ongoing treatment plan. No concerns raised.” — this takes 30 seconds to write and provides significant medicolegal protection.
-
Never alter previous entries. If you need to correct an error, add a new dated note: “Correction to note dated [date]: Antibiotic commenced was piperacillin-tazobactam, not meropenem as previously stated. — Dr. [Name], [Date/Time].”
-
Document negative findings that matter. “No signs of pneumothorax post-CVC insertion (chest X-ray reviewed)” is more useful than silence, because if pneumothorax is later discovered, the silence could be interpreted as a failure to check.
-
Use severity scores. APACHE II at admission and daily SOFA scores provide objective, standardised documentation of illness severity that is accepted by both insurance companies and courts.
Conclusion
Medicolegal documentation in ICU practice is not about creating a defensive shield after the fact — it is about building a clinical record that accurately reflects the care provided, the reasoning behind clinical decisions, and the communication with the patient’s family. A well-documented ICU record is the single most powerful tool a doctor has in any medicolegal proceeding.
For ICU doctors in India, the investment in structured, contemporaneous, complete documentation is not optional — it is the baseline standard of professional practice.
Tools like Rivara Health’s ICU Summary Generator support this by providing structured templates for daily notes, automated severity scoring, timestamped append-only entries, and AI-generated summaries that synthesize the complete clinical record into a TPA-ready document.
Related reading: How to Write an ICU Death Summary | SOFA Score in ICU: Complete Guide for Clinicians
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Reduce ICU Documentation Time by 90%
Generate medicolegal-grade ICU discharge summaries in under 2 minutes. Built for Indian hospitals, designed for TPA compliance.