In most hospitals, an ICU stay almost always involves a health insurance claim. Whether the patient is covered by a corporate group policy, a government scheme like PMJAY (Ayushman Bharat), or an individual mediclaim policy, the TPA (Third Party Administrator) will require a detailed discharge summary before processing the claim.
This document is the most important piece of paperwork the treating ICU doctor will produce. Incomplete or poorly structured summaries are the single most common cause of delayed or rejected ICU claims.
This guide covers every element a TPA-ready ICU discharge summary must include, explains why each element matters, and provides practical documentation strategies for busy ICU clinicians.
What Is a TPA and Why Does Your Documentation Matter?
A Third Party Administrator is an insurance intermediary that processes health insurance claims on behalf of insurance companies. In India, registered TPAs include organisations like Medi Assist, Paramount, MD India, Health India, and East West Assist, among others.
When your patient is discharged from the ICU, the hospital submits the claim package to the TPA. A medical reviewer at the TPA assesses whether:
- The ICU admission was medically necessary
- The duration of ICU stay was clinically justified
- The procedures billed were actually performed and documented
- The medications billed are reflected in the clinical notes
- The costs are consistent with the documented clinical severity
Your discharge summary is the primary document the TPA reviewer reads. Everything else — lab reports, imaging, operation notes — is supplementary evidence.
If the discharge summary is incomplete, the reviewer will either reject the claim outright or request a detailed resubmission — adding weeks to the process and significant administrative burden on the hospital billing team.
The 12 Required Elements of a TPA-Ready ICU Discharge Summary
1. Patient Identification
Required: Full name, age, sex, hospital admission number, date of admission, date of discharge (or date and time of death), ward, treating consultant.
Basic identification errors cause administrative rejections before the medical review even begins. Ensure these details match exactly between the discharge summary, billing documents, and the insurance policy — even minor name spelling discrepancies can trigger a rejection.
2. Admission Diagnosis and Clinical Indication for ICU
Required: The primary admission diagnosis (ICD-10 code where possible), the specific clinical indication for ICU level care, and the expected benefit of ICU admission versus general ward management.
“Patient admitted with Acute Respiratory Failure secondary to bilateral community-acquired pneumonia (ICD-10: J18.1), with PaO₂/FiO₂ ratio of 210 on FiO₂ 0.5, requiring mechanical ventilation support. ICU admission indicated for invasive ventilatory management and haemodynamic monitoring.”
“ICU admission for further management” is not a clinical indication. The TPA reviewer needs to understand specifically why the ICU level of care was required and why a general ward bed was insufficient. Vague indications are one of the top 3 rejection triggers.
3. Comorbidities and Pre-existing Conditions
Required: All relevant pre-existing medical conditions with disease duration where known.
“Background history of Type 2 Diabetes Mellitus (15 years, on oral hypoglycaemics), Hypertension (8 years, on amlodipine 5mg), and Chronic Kidney Disease Stage 3 (baseline creatinine 1.8 mg/dL).”
Comorbidities justify a more prolonged and complex ICU course. A diabetic patient with community-acquired pneumonia is expected to have slower recovery than a previously healthy patient with the same condition. Undocumented comorbidities make the ICU course appear unexpectedly complicated, raising flags with reviewers.
4. Clinical Course — Day-by-Day Narrative
Required: A coherent narrative of the clinical course, covering significant events, clinical changes, and management decisions throughout the ICU stay.
This is the most important and most commonly inadequate section of ICU discharge summaries.
Minimum required content by period:
- Days 1–3: Admission status, initial assessment, immediate interventions, early response to treatment
- Middle period: Significant clinical events (deteriorations, complications, changes in management)
- Final days: Trajectory toward discharge or, in the case of death, final deterioration and terminal events
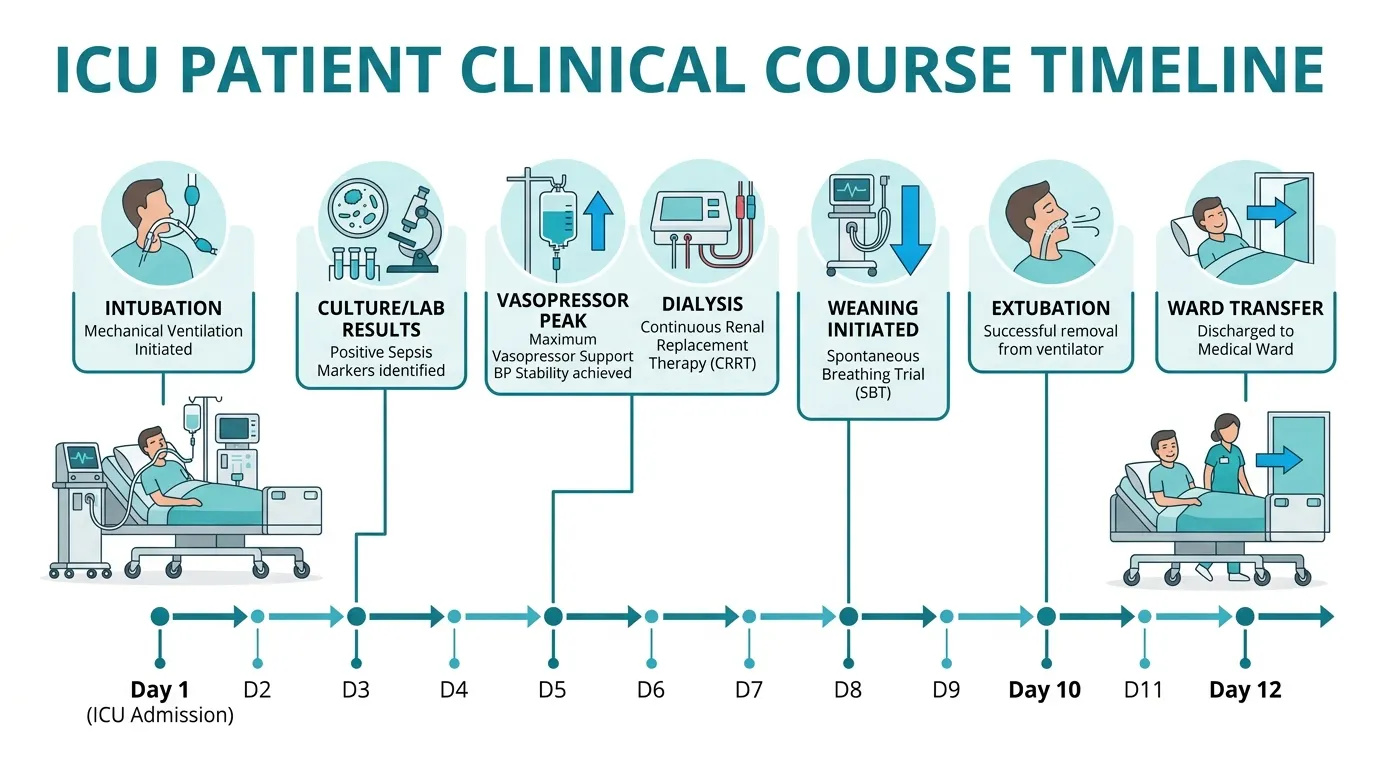
Here is an example of adequate day-by-day documentation for a 12-day ICU stay:
“On Day 1, patient was intubated for hypoxic respiratory failure and commenced on pressure-controlled ventilation (PC-AC: PC 18 cmH₂O, PEEP 8 cmH₂O, FiO₂ 0.6, RR 18). Meropenem 1g IV 8-hourly commenced empirically pending cultures.
Day 3: Blood cultures returned Klebsiella pneumoniae (ESBL-producing). Antibiotic regimen de-escalated to Ertapenem 1g IV 24-hourly per sensitivity. Haemodynamic status worsened; norepinephrine commenced at 0.05 µg/kg/min.
Day 5: Vasopressor requirement peaked at norepinephrine 0.15 µg/kg/min. Creatinine 3.2 mg/dL (baseline 0.9). CVVHDF commenced for acute renal replacement therapy.
Day 8: Vasopressors successfully weaned. Creatinine trending to 2.1 mg/dL. Spontaneous breathing trial initiated.
Day 12: Transferred to general ward on room air with SpO₂ 96% on FiO₂ 0.28 via Venturi mask.”
The TPA reviewer is checking whether the ICU stay duration was justified by the documented clinical course. A 12-day ICU stay with a detailed narrative showing initial critical illness, complications, and gradual recovery is far easier to approve than the same stay documented as “Patient admitted with pneumonia, treated with antibiotics, gradually improved, discharged.”
5. Procedures Performed
Required: Every significant procedure with date performed, indication, and outcome.
Standard procedures to document include:
- Endotracheal intubation (date, method, indication, tube size)
- Mechanical ventilation (dates commenced and weaned, mode, key parameters)
- Central venous catheter insertion (date, site, indication)
- Arterial line insertion (date, site)
- Urinary catheterisation (date)
- Nasogastric tube insertion (date)
- Renal replacement therapy (dates, modality — IHD vs CRRT vs CVVHDF)
- Bronchoscopy (date, indication, findings)
- Chest drain (date, indication, output)
- Blood transfusions (number of units, indication)
- Tracheostomy (date, indication)
- Surgical procedures (with operation notes cross-referenced)
Procedures carry significant billing implications. A TPA reviewer who sees a bill for central venous catheter placement but no documentation of the procedure in the discharge summary will flag this as a discrepancy — and may reject the entire claim pending clarification.
6. Mechanical Ventilation Details
Required: Start date, mode of ventilation, key initial parameters, changes over the course of the stay, weaning strategy, and extubation date.
“Mechanical ventilation commenced Day 1. Initial settings: PC-AC, PC 18 cmH₂O, PEEP 8 cmH₂O, FiO₂ 0.6, RR 18. PaO₂/FiO₂ ratio 160 on Day 1 (moderate ARDS). FiO₂ weaned progressively as oxygenation improved. Spontaneous breathing trials commenced Day 8. Successful extubation Day 10 after CPAP trial with satisfactory parameters.”
Ventilator days are one of the primary drivers of ICU billing. TPA reviewers expect detailed documentation to justify each ventilator day. “Patient was on ventilator for 8 days” without any parameter documentation is insufficient and frequently triggers manual review or rejection.
Daily notes that document themselves — in 3 minutes
Rivara Health's structured daily note captures ventilator settings, vasopressor doses, SOFA components and lab values in one place — then builds the discharge summary automatically.
7. Medication Documentation
Required: All significant medications administered during the ICU stay, including dose, route, duration, and indication.
At minimum, document:
- Antibiotics (agent, dose, duration, and culture-sensitivity rationale for choice)
- Vasopressors (agent, peak dose, total duration)
- Sedation and analgesia (agents, mode — continuous infusion vs PRN)
- Anticoagulants (indication, dose, monitoring)
- Insulin infusion (if used — rate, target glucose range)
- Total parenteral nutrition or enteral feeding
- Specific high-cost drugs (colistin, antifungals, IVIG, biologics)
Medication costs form a significant part of ICU bills. Antibiotics like meropenem, linezolid, colistin, and antifungals attract particular scrutiny. Each must be traceable to a clinical indication — a positive culture, a documented clinical deterioration, or an infectious disease consultation.
8. Laboratory and Investigations
Required: Key laboratory trends, not a copy of every lab report. Relevant results include:
- Serial creatinine and eGFR (for renal function trend)
- Serial bilirubin (hepatic function)
- Serial haemoglobin and platelet count (for transfusion justification and coagulopathy)
- Culture reports with organism and sensitivity
- Procalcitonin or other infection markers (if used)
- Arterial blood gas results (key time points)
- Troponin, BNP (if cardiac involvement)
- CT/MRI/X-ray findings and dates
9. SOFA and Severity Scores
Required: SOFA score at admission, peak SOFA score during the stay (with date), and SOFA score at discharge or time of death.
If APACHE-II was calculated, include admission APACHE-II and predicted mortality.
For more on SOFA score documentation — including reference ranges, component-by-component calculation, and what TPA reviewers specifically look for — see our complete SOFA score guide for ICU clinicians.
10. Complications
Required: All complications arising during the ICU stay, with dates, severity, and management.
Common ICU complications to document:
- Ventilator-associated pneumonia (VAP)
- Catheter-associated urinary tract infection (CAUTI)
- Central line-associated bloodstream infection (CLABSI)
- Acute kidney injury (AKI) — stage per KDIGO criteria
- Delirium
- Pressure ulcers
- Deep vein thrombosis
- Pneumothorax (if intercostal drain placed)
- Cardiac arrhythmias requiring treatment
Complications that arise during the ICU stay justify both the extended duration of care and the additional costs of managing them. Undocumented complications that were clearly treated (e.g., a bill for colistin with no documented carbapenem-resistant infection) raise serious red flags with TPA reviewers.
11. Outcome and Condition at Discharge
For discharge to ward or home:
“Patient transferred to general ward in stable condition. Alert and oriented. Afebrile. Tolerating oral diet. SpO₂ 96% on room air. Wound healing satisfactorily.”
For death:
“Despite maximum supportive care including mechanical ventilation, vasopressors, and renal replacement therapy, patient’s condition continued to deteriorate. Death pronounced at 14:35 on [date]. Immediate cause of death: Refractory septic shock. Underlying cause: Gram-negative bacteraemia (ESBL Klebsiella pneumoniae). Family counselled and expressed understanding.”
12. Attending Doctor Signature and Stamp
Required: Consultant signature, designation, and hospital stamp. Many TPA companies now also require the resident’s countersignature.
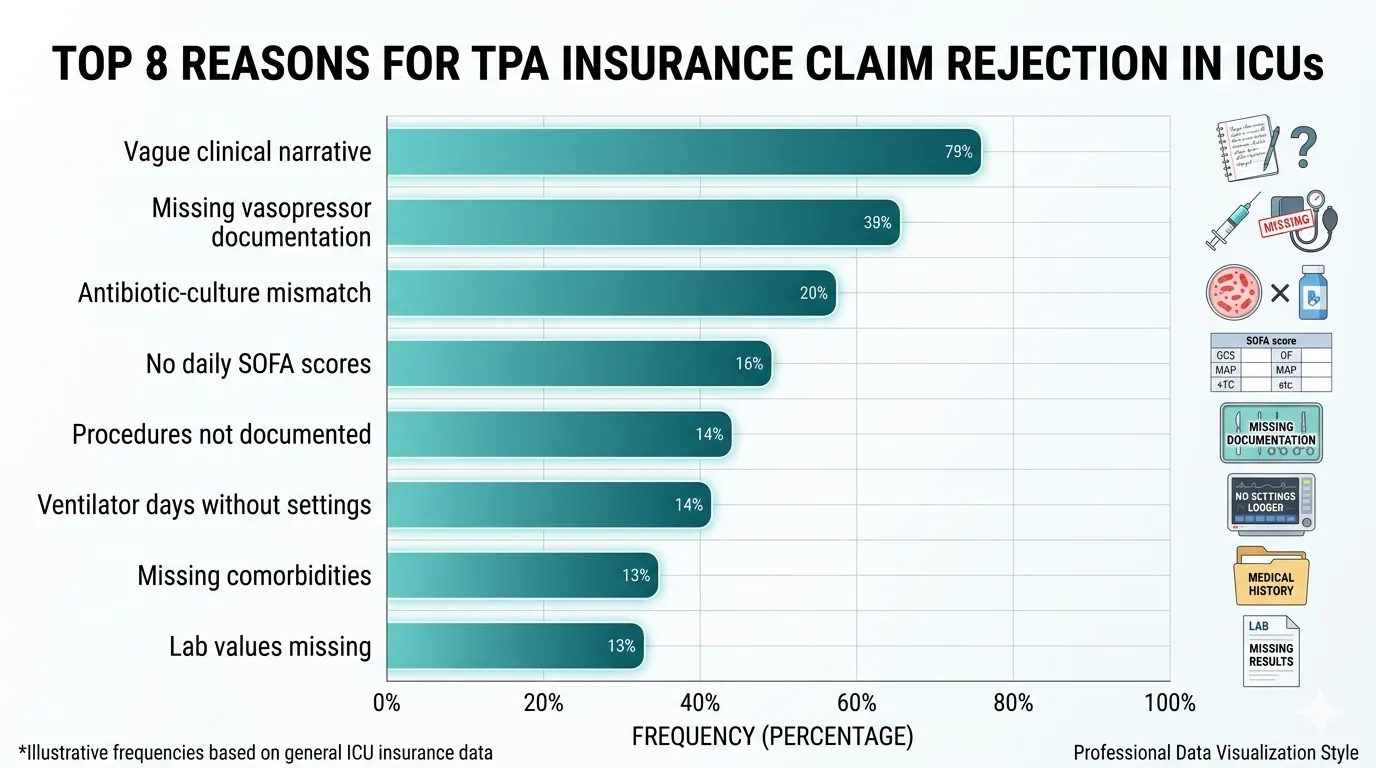
Most Common Reasons for TPA Rejection of ICU Claims
Based on common ICU billing disputes, the most frequent reasons for TPA rejection or downgrade are:
| # | Rejection Reason | How to Prevent |
|---|---|---|
| 1 | Vague clinical course narrative | Write day-by-day with specific clinical events |
| 2 | Missing vasopressor documentation | Record agent + dose in µg/kg/min + timing |
| 3 | Antibiotic-culture mismatch | Link every antibiotic to a culture or clinical rationale |
| 4 | No daily SOFA scores | Score every day, backed by documented lab values |
| 5 | Procedures billed but not documented | Document every procedure with date and indication |
| 6 | Ventilator days without settings | Record mode and key parameters daily |
| 7 | Comorbidities not documented | Document all relevant history on admission |
| 8 | Lab values missing from notes | Include key lab values in daily notes, not just lab reports |
Every rejection reason in the table above is a documentation failure, not a clinical one. The patient was genuinely ill, the care was genuinely provided, the costs were genuinely incurred — but the documentation didn’t reflect it. This is the gap AI-assisted structured documentation is designed to close.
Eliminate TPA rejections before they happen
Rivara Health's ICU Summary Generator captures all 12 required elements automatically — from daily notes to a complete, audit-proof discharge summary in under 2 minutes.
How Rivara Health’s ICU Summary Generator Addresses These Issues
Rivara Health’s ICU Summary Generator was built specifically to prevent these documentation failures. The daily note structure ensures that all relevant clinical parameters — vasopressor doses, ventilator settings, SOFA score components, lab values — are captured systematically.
When the AI generates the discharge summary, it references all of this structured data to produce a narrative that covers every element listed in this guide. The result is a discharge summary that:
- Includes daily SOFA scores backed by documented lab values
- Reflects vasopressor doses with timing
- Documents the clinical course with adequate day-by-day detail
- Covers complications and their management
- Meets the documentation standard expected by TPA reviewers
The ICU Discharge Summary Generator is free to use. Learn more about how AI is transforming ICU discharge documentation in India.
Related reading: SOFA Score in ICU: Complete Guide for Clinicians | How AI Is Transforming ICU Discharge Documentation
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Reduce ICU Documentation Time by 90%
Generate medicolegal-grade ICU discharge summaries in under 2 minutes. Built for Indian hospitals, designed for TPA compliance.