Writing a death summary is one of the most challenging documentation tasks an ICU doctor faces. Unlike a discharge summary — where the patient has improved and the narrative has a natural resolution — a death summary must document the final clinical trajectory, the exact circumstances of death, and the complete chain of causation. It must withstand scrutiny from insurance reviewers, hospital administration, and, in some cases, legal authorities.
In Indian ICUs, where mortality rates for critically ill patients can range from 20% to 40% depending on case mix, death summaries are a routine part of clinical practice. Yet many doctors receive no formal training on how to write them. The result is documentation that is often incomplete, legally vulnerable, and inadequate for TPA insurance claim processing.
This guide covers every element an ICU death summary must include, how to structure the cause-of-death chain correctly, and how to document family counselling and end-of-life decisions.

Why Death Summaries Require Special Attention
A discharge summary documents clinical improvement. A death summary documents clinical deterioration leading to an irreversible outcome. This fundamental difference creates several additional requirements:
Medicolegal scrutiny. Death summaries are far more likely to be reviewed in legal proceedings than discharge summaries. Families, lawyers, and consumer courts will examine the document for evidence of delayed treatment, inadequate care, or failure to inform the family.
Insurance complexity. TPA reviewers apply heightened scrutiny to death claims. The insurance payout is typically higher (covering the entire ICU stay without the possibility of step-down or early discharge), and the documentation must justify every intervention and every day of ICU care.
Emotional context. The family is grieving. A clear, complete death summary that explains the clinical course and cause of death can provide closure. An incomplete or confusing summary can fuel suspicion and conflict.
In medicolegal disputes, the death summary is the single most important document. If it is incomplete, inconsistent, or written hastily, it will be interpreted unfavorably — regardless of the quality of care provided. The documentation is the legal record of what happened.
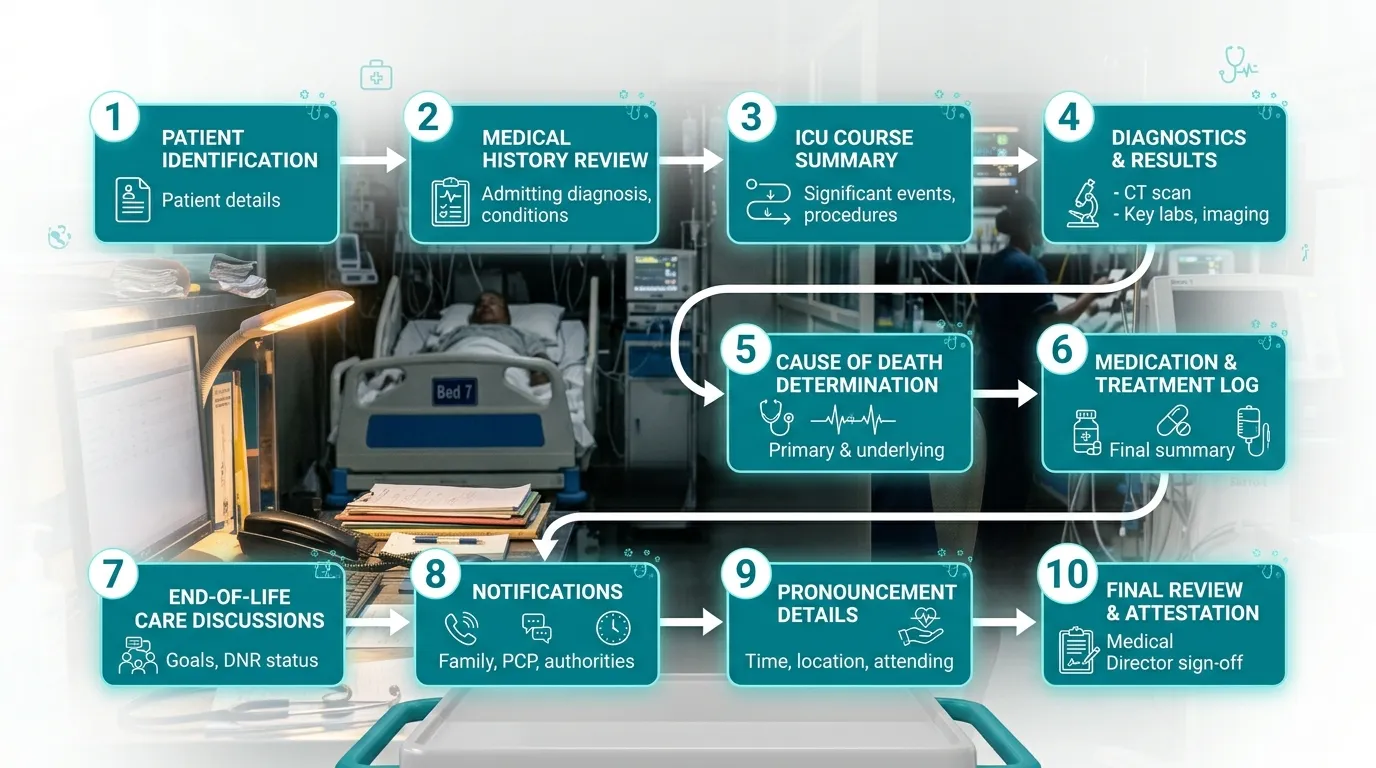
The 10 Essential Elements of an ICU Death Summary
1. Patient Identification and Admission Details
Required: Full name, age, sex, hospital number, date and time of ICU admission, treating consultant, and the source of admission (emergency department, operation theatre, ward transfer, or inter-hospital transfer).
Include the time of ICU admission, not just the date. In medicolegal reviews, the time interval between emergency presentation and ICU admission is often scrutinised — delays in ICU transfer can become a point of contention.
2. Admission Diagnosis and Clinical Indication for ICU
Required: The primary diagnosis at the time of ICU admission, any differential diagnoses being considered, and the specific clinical indication for ICU-level care.
“Admitted to ICU with septic shock secondary to perforated duodenal ulcer (post-operative Day 0), requiring invasive mechanical ventilation and vasopressor support. APACHE II score at admission: 26 (predicted mortality ~55%).”
State the severity score (APACHE II or SOFA) at admission. This establishes the baseline severity and sets expectations for the outcome. A death with an admission APACHE II of 28 is clinically expected; a death with an APACHE II of 8 requires much more explanation.
3. Comorbidities and Pre-existing Conditions
Required: All relevant pre-existing medical conditions, with duration and current treatment status. This section establishes the patient’s baseline health and the pre-existing risks that contributed to the outcome.
“Background: Type 2 Diabetes Mellitus (20 years, insulin-dependent, HbA1c 9.2%), Chronic Kidney Disease Stage 4 (baseline creatinine 3.8 mg/dL, not on dialysis), Ischaemic Heart Disease (post-CABG 2019, EF 35%).”
Comorbidities are critical in death summaries for a reason that is less relevant in discharge summaries: they establish that the patient had pre-existing physiological limitations that reduced their ability to survive critical illness. This context is essential for medicolegal defense and TPA justification.
4. Complete Clinical Course Narrative
This is the most important section of a death summary and must be substantially more detailed than in a discharge summary.
Structure the narrative in three phases:
Phase 1: Initial presentation and management (Days 1–3)
- Admission clinical status, initial investigations, working diagnosis
- Immediate interventions (intubation, vasopressors, antibiotics, surgery)
- Initial response to treatment
Phase 2: ICU course (middle period)
- Significant clinical events, complications, and changes in management
- All escalations of care (new vasopressors, dialysis initiation, additional surgery)
- Culture results and antibiotic changes
- Daily severity scores showing disease trajectory
Phase 3: Terminal deterioration and death
- When the clinical trajectory shifted from potential recovery to irreversible decline
- What interventions were attempted
- When goals of care were discussed with the family
- The final hours: specific clinical events leading to death
The terminal phase documentation is where most death summaries fail. “Patient deteriorated and died despite maximum supportive care” is inadequate. Document specifically what deteriorated (refractory hypotension, worsening acidosis, cardiac arrest), what was done (adrenaline boluses, defibrillation, CPR), and the timeline.
5. Procedures and Interventions
Required: Every procedure performed, with date, time, indication, and outcome. In a death summary, procedures take on additional significance because they demonstrate the intensity of care provided.
Document in chronological order:
- Intubation and mechanical ventilation (parameters, mode changes, failed extubation attempts)
- Central venous access (site, date, indication)
- Arterial monitoring
- Vasopressor initiation and dose escalation
- Renal replacement therapy (modality, dates, indication)
- Blood and blood product transfusions
- Surgical procedures (with cross-reference to operation notes)
- Bronchoscopy, chest drains, tracheostomy
- CPR details (if attempted) — duration, drugs administered, rhythm, outcome
For CPR documentation, follow the Utstein template: time of arrest, initial rhythm, duration of CPR, drugs administered (with doses and timing), defibrillation attempts, and time of death pronouncement. Poorly documented CPR is a common target in medicolegal reviews.
6. Cause of Death — The Causal Chain
The cause of death must be documented as a causal chain, following the WHO International Form of Medical Certificate of Cause of Death (Form 4/4A) format:
Part I:
- (a) Immediate cause: The final physiological event that directly caused death
- (b) Due to (or as a consequence of): The condition leading to (a)
- (c) Due to (or as a consequence of): The underlying condition leading to (b)
- (d) Due to (or as a consequence of): The original/underlying cause
Part II: Other significant contributing conditions not directly in the causal chain
Example:
Part I: (a) Refractory septic shock with multi-organ dysfunction (b) Gram-negative bacteraemia (Carbapenem-resistant Klebsiella pneumoniae) (c) Hospital-acquired pneumonia (ventilator-associated) (d) Prolonged ICU stay for acute respiratory failure secondary to community-acquired pneumonia
Part II: Type 2 Diabetes Mellitus, Chronic Kidney Disease Stage 4
Never write a single-line cause of death. “Cause of death: Cardiac arrest” is technically true for every death and is meaningless. Cardiac arrest is the mechanism, not the cause. The causal chain must trace back to the underlying disease process.
The causal chain should be internally consistent. If (a) is “refractory septic shock,” then (b) must explain the source of sepsis, and (c)/(d) should explain how the patient developed that source. A chain that jumps from septic shock to “diabetes mellitus” without the intervening steps will be questioned.
From daily notes to a complete death summary — automatically
Rivara Health captures the full ICU clinical course in structured daily notes, then generates a comprehensive death summary with causal chain and severity scores.
7. Family Counselling Documentation
Family counselling documentation is critical in death summaries and is frequently inadequate.
Document for every counselling session:
- Date and time of the counselling
- Who was present (family member names and relationship to patient, plus which doctors were present)
- What was communicated (diagnosis, prognosis, treatment options, expected outcomes)
- Family’s response (understanding expressed, questions asked, decisions made)
- Whether the family acknowledged the gravity of the situation (e.g., “Family counselled regarding poor prognosis and high likelihood of mortality. Family expressed understanding.”)
In consumer court disputes, the most common family allegation is: “We were never told the patient might die.” If counselling is not documented, it effectively never happened — regardless of how many conversations actually took place. Document every counselling session, including informal bedside conversations where prognosis was discussed.
Key counselling milestones to document:
- At admission: Initial diagnosis, severity, expected ICU course
- At escalation: When new complications arise or care is escalated (dialysis, additional surgery)
- At deterioration: When the clinical trajectory shifts unfavorably
- Before withdrawal/withholding of care: If goals-of-care discussions lead to limitation of treatment
- At or near the time of death: Final communication about the patient’s condition
8. Do-Not-Resuscitate (DNR) and Goals-of-Care Documentation
If goals-of-care discussions took place, document:
- When the discussion was initiated and by whom
- What options were discussed (full code, limited resuscitation, comfort care)
- The family’s decision and whether it was unanimous
- Whether the patient had previously expressed wishes (advance directive, verbal instructions)
- Written consent if DNR was agreed upon
DNR documentation must be crystal clear. A vaguely documented DNR (“family not keen on aggressive measures”) is not a valid DNR order and exposes the treating team to legal risk. Document the specific interventions that were withheld or withdrawn, the family’s explicit consent, and the clinical rationale.
9. Time and Circumstances of Death
Required: Exact time of death, who pronounced death, and the clinical circumstances.
“At 03:45 on 15-Mar-2026, patient developed sudden bradycardia progressing to asystole. CPR was initiated at 03:47. Despite 30 minutes of advanced cardiac life support including 4 doses of adrenaline 1mg IV, 2 doses of atropine 0.6mg IV, and continuous chest compressions, there was no return of spontaneous circulation. Death was pronounced at 04:17 by Dr. [Name], Consultant Intensivist.”
Alternatively, if DNR was in place:
“Patient’s clinical condition continued to deteriorate with progressive hypotension (MAP 38 mmHg) and worsening metabolic acidosis (pH 7.02, lactate 14.2 mmol/L) despite maximum vasopressor support. As per the previously documented family decision for limited resuscitation, CPR was not initiated. Death was pronounced at 14:22 on 15-Mar-2026.”
Always document the exact time of death pronouncement and the name and designation of the doctor who pronounced it. In medicolegal reviews, the time of death is a critical data point — especially if there are questions about the timeline of events.
10. Post-Mortem and Body Handover
Document whether:
- Post-mortem was advised to the family and their decision
- If post-mortem was declined, document the family’s refusal
- Time of body handover to the family or mortuary
- Whether the death was reported to the police (mandatory for medico-legal cases — brought dead, deaths within 24 hours of admission, deaths under suspicious circumstances, deaths due to poisoning, burns, or assault)
Don't let documentation gaps undermine the care you provided
Rivara Health's structured daily notes capture every clinical event, procedure, and family interaction — making death summary generation thorough and auditable.
Common Mistakes in ICU Death Summaries
1. Vague Cause of Death
Wrong: “Cause of death: Multi-organ failure” Right: Provide the complete causal chain from immediate cause back to the underlying disease.
2. Missing Terminal Event Documentation
Wrong: “Patient deteriorated and expired.” Right: Document the specific terminal event (cardiac arrest, refractory hypotension, respiratory failure), what was done, and the timeline.
3. No Family Counselling Records
If there is no documentation of family counselling, the legal presumption is that the family was not informed. Document every conversation.
4. Incomplete CPR Documentation
If CPR was performed, document it using the Utstein template: time of arrest, initial rhythm, interventions, duration, and outcome. “CPR was done but was unsuccessful” is insufficient.
5. Single-Line Clinical Course
A 15-day ICU stay summarised as “Patient was treated with ventilator, antibiotics, and vasopressors but did not improve” will not survive TPA review or medicolegal scrutiny. The day-by-day narrative is non-negotiable.
6. Inconsistent Severity Scores
An admission APACHE II of 8 with death on Day 3 raises questions. If the patient genuinely deteriorated rapidly, the daily SOFA scores should document this trajectory. Severity scores must tell a consistent story.
Death Summary vs Discharge Summary: Key Differences
| Element | Discharge Summary | Death Summary |
|---|---|---|
| Outcome section | Condition at discharge, follow-up plan | Time of death, circumstances, cause-of-death chain |
| Clinical course detail | Important but moderate | Must be highly detailed with terminal phase |
| Family counselling | Brief or omitted | Must document all counselling sessions |
| CPR documentation | N/A | Required if CPR was attempted |
| Medicolegal scrutiny | Moderate | High |
| Cause-of-death chain | N/A | Required (WHO Part I/Part II format) |
| DNR documentation | Rare | Common and critical |
| Post-mortem documentation | N/A | Required (whether advised, accepted, or declined) |
Conclusion
An ICU death summary is not just a clinical document — it is a medicolegal record, an insurance claim document, and often the final piece of communication between the treating team and the patient’s family. It must be thorough, accurate, and structured to withstand scrutiny from multiple stakeholders.
For ICU doctors, investing time in a well-documented death summary is one of the most important things you can do to protect your patients’ families, your colleagues, and yourself.
Tools like Rivara Health’s ICU Summary Generator capture structured clinical data throughout the ICU stay — including daily SOFA scores, procedures, medications, and family counselling notes — making it possible to generate a comprehensive death summary that covers every element described in this guide.
Related reading: ICU Discharge Summary for TPA Insurance Claims | How AI Is Transforming ICU Discharge Documentation
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Reduce ICU Documentation Time by 90%
Generate medicolegal-grade ICU discharge summaries in under 2 minutes. Built for Indian hospitals, designed for TPA compliance.