ICU documentation is the foundation of critical care practice. Every clinical decision, every dose titration, every family conversation — if it is not documented, it functionally did not happen. Yet documentation in the intensive care unit is uniquely challenging: patients are complex, clinical situations evolve rapidly, and the physician’s time is stretched between bedside care, procedures, and administrative demands.
Poor ICU documentation has measurable consequences. Studies show that incomplete discharge summaries are associated with increased adverse events after ICU transfer. Insurance claim denials frequently trace back to documentation gaps rather than clinical shortcomings. And in medicolegal proceedings, courts assess the quality of care through the quality of the written record.
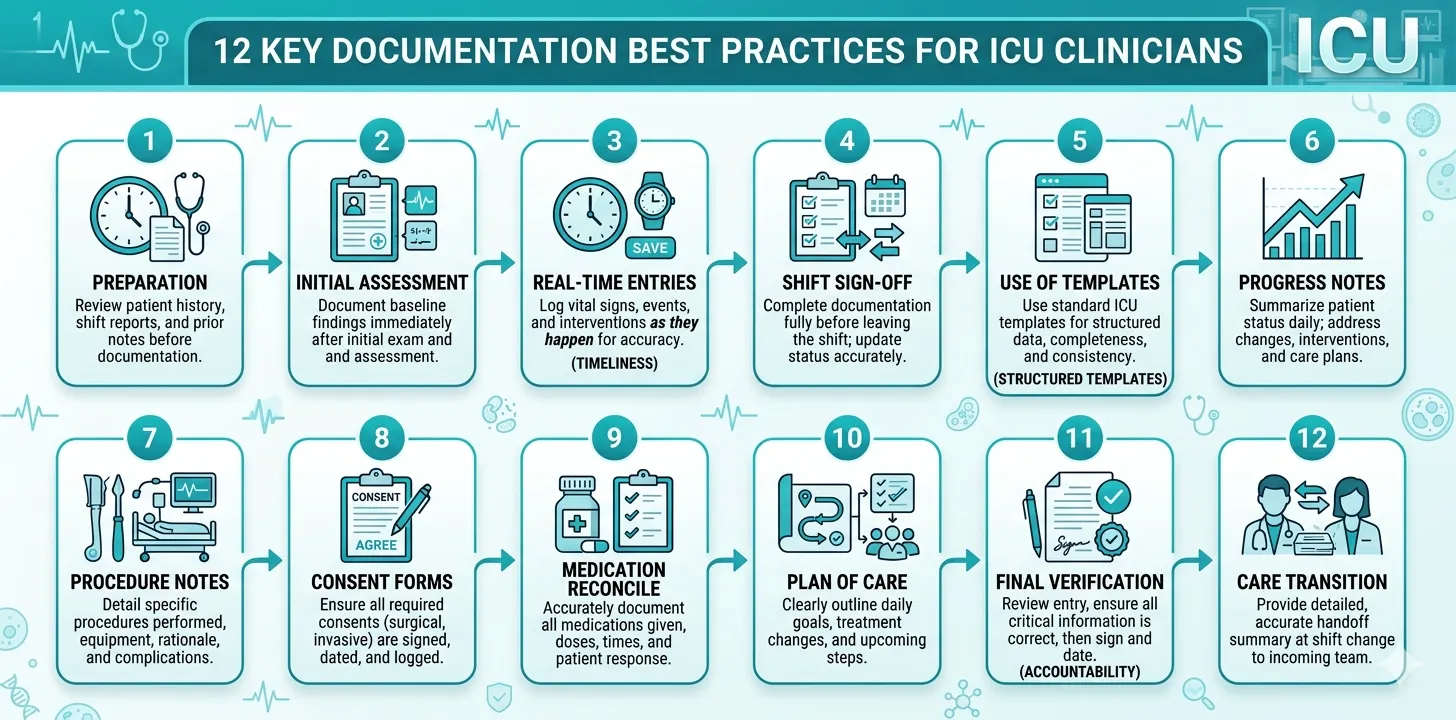
These 12 rules distil the principles that separate defensible, clinically useful ICU documentation from records that create risk. They apply regardless of your institution, your country, or whether you work on paper or an electronic health record.

Rule 1: Document in Real Time — Not from Memory
The single most impactful change any intensivist can make to their documentation quality is reducing the time gap between a clinical event and its documentation. Notes written hours after the fact suffer from recall bias, omitted details, and conflation of events. Notes written the next day are unreliable. Notes written at discharge, reconstructing a two-week ICU stay from fragmented recollections, are dangerous.
Real-time documentation does not mean writing a full progress note after every intervention. It means capturing key data points — a procedure, a medication change, a clinical deterioration, a family discussion — at or near the time they occur. These contemporaneous entries form the raw material for progress notes and, ultimately, the discharge summary.
In medicolegal analysis, contemporaneous records carry significantly more weight than retrospective documentation. A note timed at 02:30 describing a desaturation event and the response to it is far stronger evidence than a retrospective note written at 08:00 stating “desaturation overnight — managed appropriately.”
The practical barrier is time. Structured data entry — selecting from predefined fields rather than composing free text — reduces the time cost of real-time documentation to minutes per entry. This is one reason structured daily note systems outperform narrative-only workflows in documentation completeness studies.
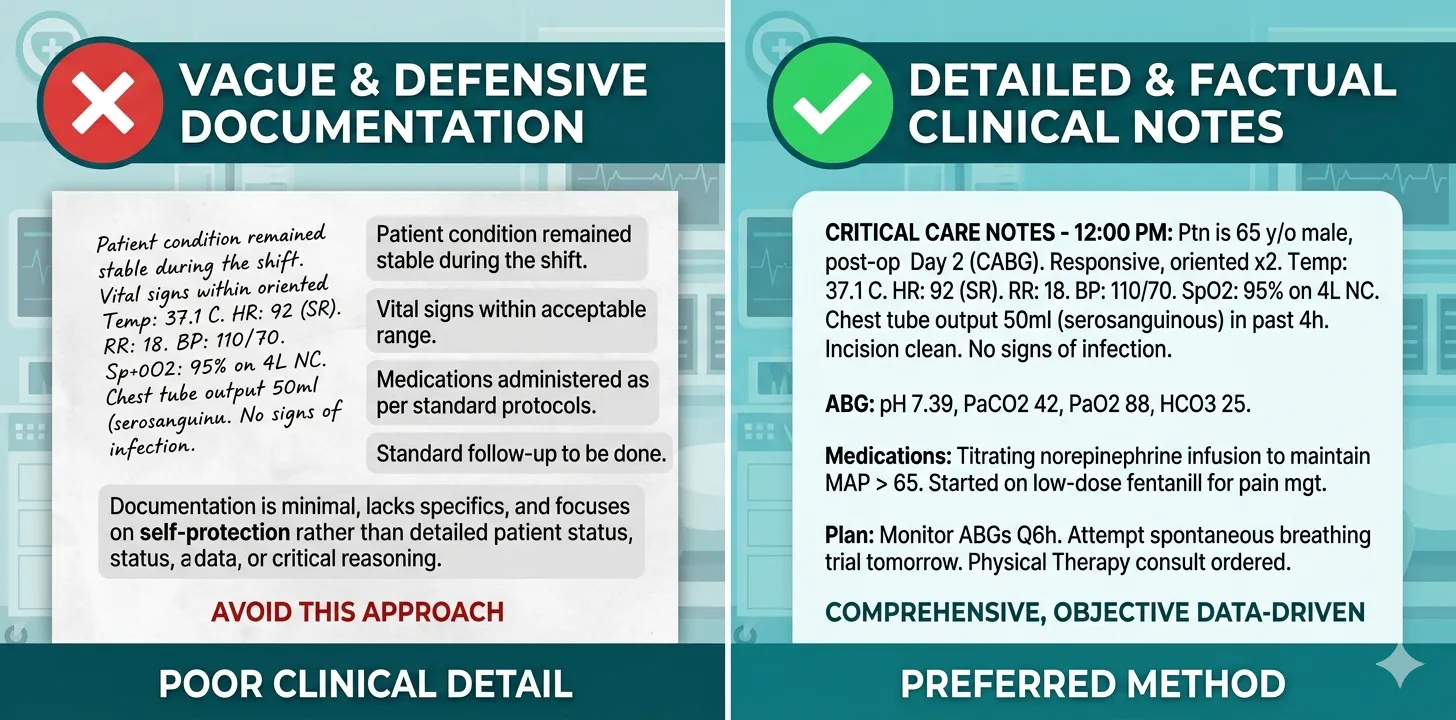
Rule 2: Be Objective and Precise — Avoid Subjective Language
ICU documentation must be grounded in objective, measurable data. Subjective phrases like “patient looks better,” “doing well,” or “seems comfortable” carry no clinical or legal weight. They cannot be verified, compared, or used to justify clinical decisions.
Replace subjective language with quantifiable observations:
| Subjective (Avoid) | Objective (Use Instead) |
|---|---|
| “Patient looks better" | "Temperature normalised (36.8°C), MAP 78 mmHg off vasopressors, WBC trending down (14 → 9.2 × 10⁹/L)" |
| "Comfortable on current settings" | "RASS −1, no accessory muscle use, RR 16, SpO₂ 97% on PS 10/PEEP 5" |
| "Poor urine output" | "Urine output 15 mL/hr over the past 6 hours (total 90 mL)" |
| "Improving" | "SOFA score improved from 14 (Day 1) to 9 (Day 4)” |
A practical test: could another clinician, reading your note without seeing the patient, form an accurate clinical picture? If your note requires the reader to interpret what “better” or “worse” means, it lacks the precision required for ICU-level documentation.
This principle extends to describing complications. “Patient had a difficult intubation” is vague. “Intubation required three attempts; Grade 3b Cormack–Lehane view on direct laryngoscopy; successfully intubated with video laryngoscope, 7.5 mm ETT, at 23 cm at the lip” is defensible.
Rule 3: Document the Clinical Reasoning — Not Just the Outcome
Recording what you did is necessary. Recording why you did it is what makes the documentation clinically and legally robust. The clinical reasoning behind a decision is often more important than the decision itself — especially when the outcome is adverse.
Consider antibiotic escalation. A note stating “changed to meropenem” documents the action but not the thought process. A note stating “Escalated from piperacillin-tazobactam to meropenem due to clinical deterioration (rising lactate, new vasopressor requirement) despite 72 hours of initial therapy; pending cultures; covering for possible ESBL-producing organism given local resistance patterns” makes the reasoning visible and defensible.
Courts do not judge clinicians for adverse outcomes alone — they judge whether the clinical reasoning was sound given the information available at the time. Documentation that captures the reasoning demonstrates that a thoughtful, systematic approach was taken, even when the outcome was not ideal.
This applies equally to decisions not to intervene. If you decided against intubation despite borderline respiratory parameters, document why: “Maintained on NIV given improving trend in blood gas over 4 hours (pH 7.28 → 7.33, PaCO₂ 62 → 51 mmHg), patient cooperative, no accessory muscle use; intubation threshold discussed with team — to proceed if pH falls below 7.25 or patient shows fatigue.” This is far stronger than no documentation of the decision at all.
Rule 4: Record Severity Scores Daily — With Component-Level Detail
Severity scoring systems — particularly the SOFA score and APACHE II — serve multiple purposes in ICU documentation. They quantify illness severity at admission, track the trajectory of organ dysfunction over time, justify the level of care provided, and provide standardised data for benchmarking and quality reporting.
A SOFA score recorded without component values is nearly useless. “SOFA 14” tells the reader the patient is critically ill but not which organs are failing. “SOFA 14 (Resp 4, Coag 1, Hepatic 2, Cardio 4, CNS 1, Renal 2)” provides a complete picture of multi-organ dysfunction that any clinician can interpret immediately.
Insurance reviewers and TPA auditors routinely cross-check SOFA scores against documented lab values and clinical parameters. A cardiovascular SOFA of 4 that is not supported by documented vasopressor doses, or a renal SOFA of 3 without a corresponding creatinine value in the notes, will be flagged. Scores must always be traceable to source data.
Best practice is to calculate and document the SOFA score at a consistent time each day — typically during the morning ward round. This creates a reliable severity trajectory that is clinically meaningful and administratively defensible.
Rule 5: Maintain a Complete and Accurate Medication Record
Medication documentation in the ICU extends far beyond a prescription list. Vasopressor infusions, sedation protocols, antibiotic timelines, and fluid resuscitation all require dose-level, time-stamped documentation that captures not just what was given but when, how much, and why changes were made.
Key principles for ICU medication documentation:
- Vasopressors and inotropes: Document the agent, dose in standardised units (µg/kg/min, not mL/hr), peak dose, and weaning trajectory. “Norepinephrine started at 0.05 µg/kg/min, peak 0.25 µg/kg/min on Day 2, weaned and stopped Day 5” tells the full haemodynamic story.
- Antimicrobials: Document each agent with its indication, start date, intended duration, and any escalation or de-escalation decisions with rationale. Link antibiotic changes to culture and sensitivity results.
- Sedation: Record the agent, target RASS score, and any dose adjustments. Note sedation holds and neurological assessments performed during holds.
- Fluids and nutrition: Document resuscitation volumes, maintenance fluids, enteral and parenteral nutrition with caloric targets and achieved intake.
When documenting vasopressor doses, always use weight-based units (µg/kg/min) rather than infusion rates (mL/hr). The infusion rate depends on the drug concentration, which varies between institutions and even between batches. Weight-based dosing is the universal standard and the only format that is clinically interpretable across settings.
Tired of reconstructing medication timelines at discharge?
Rivara Health captures vasopressor doses, antibiotic changes, and sedation protocols as part of structured daily ICU notes — building the medication record automatically.
Rule 6: Document Every Procedure at the Time It Is Performed
Every procedure performed in the ICU must have a contemporaneous procedure note. This is non-negotiable for both clinical and medicolegal reasons. A central venous catheter inserted without a procedure note, followed by a catheter-related bloodstream infection, creates a documentation gap that no retrospective note can adequately fill.
A complete ICU procedure note includes:
- Date and time of the procedure
- Indication — why this procedure was necessary
- Informed consent — obtained from patient or next of kin, or waived due to emergency
- Technique — approach, equipment, aseptic precautions
- Findings — what was seen or encountered
- Complications — any immediate complications, or explicitly “no immediate complications”
- Confirmation — method of confirming correct placement (ultrasound, chest X-ray, blood gas)
- Operator — who performed the procedure and who supervised
For intubation, include the laryngoscopy grade (Cormack–Lehane), number of attempts, drugs used for induction and paralysis, ETT size and depth at the lip, and confirmation method. For central lines, include the site, laterality, number of attempts, use of ultrasound guidance, and post-insertion CXR findings. These details matter enormously in any subsequent review of the procedure.
Rule 7: Write for Your Downstream Audience
An ICU note is not just for the ICU team. The discharge summary will be read by ward physicians, rehabilitation specialists, primary care doctors, insurance reviewers, and potentially lawyers and judges. Each audience has different needs, but all require clarity, completeness, and logical structure.
Write as though the reader has no prior knowledge of the patient. Avoid abbreviations that are not universally understood — what is standard in your unit may be unintelligible to a general practitioner reviewing the record months later. Spell out diagnoses, procedures, and drug names on first use.
The complete guide to ICU discharge summaries covers the specific structure and content requirements for discharge documentation in detail. The principle here is broader: every note you write during the ICU stay should be written with the awareness that it may be the only record someone reads.
The discharge summary is often the only ICU document a downstream clinician will see. But in medicolegal proceedings, the entire clinical record — including daily progress notes, procedure notes, and nursing observations — is reviewed. Every note must stand on its own as a clear, complete, and defensible account of what happened and why.
Rule 8: Document Complications Factually — Not Defensively
When complications occur — and in intensive care, they inevitably will — the documentation must be factual, specific, and contemporaneous. State what happened, when it was identified, what was done in response, and what the outcome was.
Avoid defensive language. Phrases like “despite best efforts,” “unfortunately,” or “through no fault of the treating team” weaken the documentation rather than strengthening it. They signal anxiety rather than professionalism. A factual account of appropriate management is always stronger than a defensive narrative.
Poor documentation of a complication:
“Patient unfortunately developed VAP despite best efforts at infection control. Antibiotics were adjusted.”
Strong documentation:
“Day 7: New fever (39.2°C), rising WBC (18.4 × 10⁹/L), purulent tracheal aspirate, new right lower lobe infiltrate on CXR. Clinical diagnosis of ventilator-associated pneumonia. Tracheal aspirate sent for culture. Empiric therapy with piperacillin-tazobactam commenced pending sensitivities. VAP bundle compliance reviewed — head-of-bed elevation maintained, oral care protocol adhered to, sedation vacation performed daily.”
The second version documents the complication, the diagnostic reasoning, the immediate management, and the preventive measures that were in place. It is factually complete and medicolegally robust. For a deeper exploration of medicolegal documentation principles in the ICU, see our dedicated guide.
Rule 9: Record All Family Communication and Shared Decisions
Family communication in the ICU is a clinical activity that requires documentation with the same rigour as any procedure or treatment decision. Goals-of-care discussions, prognostic conversations, consent for procedures, and decisions about limitation of treatment must be recorded with:
- Date and time of the discussion
- Who was present — family members (by relationship), clinical staff, interpreters
- What was communicated — prognosis, treatment options, risks
- Family’s response and understanding — questions asked, concerns raised, level of agreement
- Decisions reached — full escalation, limitations, comfort care, specific requests
Undocumented family discussions are a frequent source of medicolegal disputes. Families may later claim they were not informed of risks, were not involved in decision-making, or did not consent to a course of action. Contemporaneous notes — written at the time of the discussion — are the strongest defence against such claims.
In cases involving withdrawal of life-sustaining treatment, the documentation requirements are even more stringent. Record the clinical basis for the decision, the involvement of the multidisciplinary team, the family’s understanding and agreement, and the specific plan for comfort care. Multiple documented discussions showing a process of shared decision-making are far more defensible than a single note.
Rule 10: Use Structured Templates — Do Not Rely on Free Text Alone
Free-text clinical notes allow flexibility but invite omissions. Research in the Journal of Critical Care has shown that structured documentation templates reduce documentation gaps by approximately 40% compared to free-text-only approaches. The reason is straightforward: a template with mandatory fields acts as a checklist, prompting the clinician to document items they might otherwise overlook.
Effective ICU documentation templates include structured fields for:
- Vital signs and ventilator parameters
- Fluid balance (intake, output, net balance)
- Medication changes with rationale
- Severity scores (SOFA, GCS) with component values
- Active problems list with current management
- Pending investigations and results
- Plan for the next 24 hours
Free text should supplement structured data, not replace it. The clinical course narrative, the reasoning behind a treatment change, and the nuance of a family discussion all benefit from prose. But the objective data — vitals, labs, scores, medications — should be captured in structured fields that are consistent, complete, and machine-readable.
If your unit does not have a structured daily note template, create one. Even a simple paper-based checklist that prompts for SOFA score, fluid balance, medication changes, and active problems will improve documentation completeness. Digital structured note systems take this further by auto-calculating scores and generating discharge summaries from the accumulated data.
Rule 11: Ensure Medication Reconciliation at Every Transition
Medication errors are the most common preventable adverse events in hospitalised patients, and transitions of care — ICU admission, ICU discharge, inter-facility transfer — are the highest-risk moments. Medication reconciliation at every transition point is both a patient safety imperative and a documentation requirement.
At ICU admission, document:
- Pre-admission medications — what the patient was taking before this illness, including dose, frequency, and route
- Medications held or discontinued — and the reason (e.g., “metformin held due to acute kidney injury and lactic acidosis risk”)
- New medications initiated — with indication
At ICU discharge, document:
- Current medications — the complete list the patient is leaving the ICU on
- Medications stopped during the ICU stay — and whether they should be restarted (and when)
- New medications started in the ICU — with intended duration and monitoring requirements
- Dose adjustments — any medications whose dose was changed and why
The most dangerous medication reconciliation gap is the “held and forgotten” drug. A patient’s home statin, antiplatelet, or antihypertensive may be appropriately held during the acute ICU phase but never restarted at discharge. Structured medication reconciliation at discharge — comparing the pre-admission list against the discharge list — catches these omissions before they cause harm.
Build discharge summaries from structured daily notes
Rivara Health tracks medications, procedures, and severity scores throughout the ICU stay — then generates a complete, formatted discharge summary ready for review.
Rule 12: Review, Sign, and Take Accountability
The final step in ICU documentation is review and attestation. Every note — progress note, procedure note, discharge summary — must be reviewed for accuracy, signed by the responsible physician, and attributed with a date and time. Unsigned, unattested notes carry significantly less weight in any administrative or legal review.
Review is not a formality. It is the physician’s confirmation that the documented content is accurate, complete, and reflects the care that was provided. In teaching hospitals, the supervising consultant must review and co-sign notes written by trainees, confirming both the content and the supervisory relationship.
For ICU discharge summaries, the review checklist should include:
- All procedures documented with dates and operators
- Medication list matches the patient’s current regimen
- Severity scores included with component-level values
- Culture results and antibiotic decisions recorded
- Complications listed with management
- Follow-up plan is specific and actionable
- Pending results flagged for the receiving team
In many malpractice cases, the question “Who was responsible for this patient?” becomes central. A clearly signed and attributed clinical record — with named author, supervising physician, and timestamp — establishes the chain of responsibility unambiguously. Unsigned notes invite the inference that no one took ownership of the care.
The growing role of AI in critical care documentation does not change this principle. Whether a note is written by hand, typed into an EMR, or generated by an AI system, the reviewing physician remains the author of record and bears full responsibility for its accuracy. AI accelerates the mechanical work; accountability remains human.
Bringing It All Together
These 12 rules are not independent — they form an integrated documentation workflow. Real-time capture (Rule 1) feeds structured templates (Rule 10). Objective data (Rule 2) supports severity scoring (Rule 4). Clinical reasoning (Rule 3) makes complication documentation (Rule 8) and medication records (Rule 5) defensible. And the final review (Rule 12) ensures that everything comes together in a record that is complete, accurate, and attributable.
| Rule | Core Principle | Primary Benefit |
|---|---|---|
| 1. Document in real time | Capture events as they happen | Accuracy, medicolegal weight |
| 2. Be objective and precise | Use measurable data, not subjective language | Clinical clarity, reproducibility |
| 3. Document clinical reasoning | Record the “why” behind decisions | Legal defensibility |
| 4. Record severity scores daily | SOFA/APACHE with component values | Severity tracking, insurance compliance |
| 5. Maintain complete medication records | Dose-level, time-stamped drug documentation | Patient safety, continuity |
| 6. Document every procedure | Contemporaneous procedure notes | Medicolegal protection |
| 7. Write for downstream audiences | Assume the reader has no prior context | Handoff quality, readability |
| 8. Document complications factually | No defensive language — state facts | Stronger legal position |
| 9. Record family communication | Date, attendees, content, decisions | Shared decision-making evidence |
| 10. Use structured templates | Mandatory fields reduce omissions | Completeness, consistency |
| 11. Reconcile medications at transitions | Compare pre-admission, ICU, and discharge lists | Patient safety |
| 12. Review, sign, and attest | Physician confirmation of accuracy | Accountability, legal validity |
The documentation burden in intensive care is real. These rules do not pretend otherwise. But the cost of poor documentation — in patient safety, in insurance denials, in medicolegal exposure — is far greater than the cost of doing it systematically.
Tools like Rivara Health’s ICU Summary Generator are designed to reduce the mechanical burden by collecting structured data during the stay and generating complete discharge summaries at the end. The clinical thinking — the reasoning, the judgement, the accountability — remains entirely with the treating physician. The 12 rules above apply whether you document on paper, in an EMR, or with AI assistance. They are the standard.
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Conclusion
ICU documentation is not a clerical task — it is a clinical skill. The quality of the written record directly affects patient safety during care transitions, the outcome of insurance claims, and the physician’s position in any medicolegal review. These 12 rules provide a systematic framework for documentation that is timely, objective, complete, and defensible.
The principles are universal: document in real time, use objective language, capture clinical reasoning, score severity daily, maintain accurate medication records, document procedures contemporaneously, write for your audience, handle complications factually, record family discussions, use structured templates, reconcile medications at transitions, and review everything before signing.
No single rule is sufficient on its own. Together, they create a documentation practice that protects both patients and clinicians — and produces records that stand up to any level of scrutiny.
Related reading:
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Reduce ICU Documentation Time by 90%
Generate medicolegal-grade ICU discharge summaries in under 2 minutes. Built for Indian hospitals, designed for TPA compliance.