Transferring a critically ill patient between facilities is one of the highest-risk events in intensive care medicine. The patient leaves the controlled environment of one ICU — with its established team, its familiarity with the clinical trajectory, its institutional knowledge — and arrives at another facility where nobody has seen this patient before. The ICU transfer summary is the document that bridges that gap. It is the receiving team’s only window into what has happened, what is ongoing, and what to expect next.
A poorly written transfer summary does not just create administrative friction. It creates clinical danger. Missed medication infusions, unknown allergies, undocumented procedures, ambiguous ventilator strategies — these are the gaps that cause harm during the vulnerable hours after an inter-facility transfer.
This guide covers what belongs in an ICU transfer summary, how it differs from a standard discharge summary, and how to write one that keeps the patient safe and keeps the transferring team protected.
What Is an ICU Transfer Summary?
An ICU transfer summary is a structured clinical document prepared when a critically ill patient is moved from one facility to another. Unlike a discharge summary — which documents the conclusion of an ICU stay — a transfer summary documents a patient whose care is ongoing and whose clinical trajectory is still evolving.
The distinction matters. A discharge summary looks backward: what happened, what was done, and what the outcome was. A transfer summary looks both backward and forward: what has happened so far, what the current clinical state is at this exact moment, and what the receiving team needs to do immediately upon arrival.
| Feature | ICU Discharge Summary | ICU Transfer Summary |
|---|---|---|
| Timing | End of ICU stay | Mid-course, care ongoing |
| Clinical status | Stable or improving | Often unstable or requiring active intervention |
| Medication detail | Discharge medications list | Active infusions with current rates and concentrations |
| Ventilator documentation | Summary of ventilation course | Current settings and recent changes |
| Urgency of information | Reference document | Immediate action document |
| Receiving audience | Ward team, outpatient providers | Another ICU team assuming care in real-time |
For a comprehensive guide to ICU discharge summaries and their structure, see our complete guide to ICU discharge summaries.
The transfer summary is not a medical record summary — it is a clinical handoff tool. The receiving intensivist needs to make immediate decisions about ventilator management, vasopressor titration, antibiotic timing, and monitoring priorities. Every piece of information in the transfer summary should serve that purpose.
Why ICU Transfer Summaries Are High-Stakes Documents
Patient Safety During Transitions
Inter-facility transfers are among the most dangerous moments in a critically ill patient’s trajectory. Research published in Critical Care Medicine has consistently shown that patient handoffs — particularly between institutions — are associated with increased rates of adverse events. The reasons are predictable: information loss, communication gaps, and unfamiliarity with the patient’s clinical nuances.
A transfer summary cannot eliminate these risks entirely, but it can dramatically reduce them. When the receiving team has a clear, complete, and current picture of the patient’s status, they can continue care without interruption rather than spending the first critical hours trying to reconstruct what happened.
Legal Liability for Both Facilities
The transfer of a critically ill patient creates a legally complex situation. The sending facility remains liable for the adequacy of the transfer — including the completeness of the clinical handoff. The receiving facility assumes responsibility upon acceptance but is disadvantaged if key information was not communicated.
In medicolegal proceedings following adverse outcomes during or after transfer, the transfer summary is the primary evidence of what was communicated. An incomplete summary exposes the sending team to claims of negligent handoff; a thorough one demonstrates that the standard of care was met.
For a deeper exploration of medicolegal documentation requirements in intensive care, see our guide to medicolegal documentation in the ICU.
Transfer-related litigation often hinges on a single question: did the sending team communicate the critical information the receiving team needed to provide safe care? The transfer summary is the evidence. Verbal handoffs are important, but they leave no record. The written document is what survives in court.
Regulatory and Accreditation Requirements
Most healthcare accreditation bodies — including the Joint Commission (JCAHO), the Australian Commission on Safety and Quality in Health Care, NHS England, and India’s NABH — mandate specific documentation requirements for inter-facility transfers. These typically include:
- Documented reason for transfer
- Clinical condition at the time of transfer
- Treatment provided and ongoing
- Informed consent for transfer
- Communication with the receiving facility
- Identity of the accepting physician
Failure to meet these requirements does not just create accreditation risk — it creates legal exposure and, most importantly, clinical danger.
Essential Components of an ICU Transfer Summary
An effective ICU transfer summary must cover nine domains. Unlike a discharge summary, where some sections can be relatively brief, every section of a transfer summary demands precision and currency — the information must reflect the patient’s status at the time of transfer, not hours or days earlier.
1. Patient Identification and Transfer Details
- Full patient identifiers: Name, age, sex, medical record number, and any government identification numbers required by the receiving facility
- Sending facility: Hospital name, ICU name, contact number for the transferring intensivist
- Receiving facility: Hospital name, accepting department, name of the accepting physician
- Date and time of transfer
- Reason for transfer: This must be specific — “higher level of care,” “specialist intervention not available at sending facility,” “family preference with clinical justification,” or “capacity constraints”
- Mode of transport: Ground ambulance, air ambulance, with or without physician escort
- Consent: Documented informed consent for transfer, including risks discussed with patient or family
Always include a direct contact number for the transferring intensivist — not a hospital switchboard. The receiving team will invariably have questions in the first hours after arrival, and the ability to reach the physician who actually managed the patient is invaluable.
2. Reason for ICU Admission and Primary Diagnosis
State the original reason for ICU admission and the current working diagnosis. These may differ — a patient admitted for post-operative monitoring who subsequently developed septic shock has a different clinical trajectory than originally anticipated.
Include:
- Primary diagnosis at the time of transfer (not just the admission diagnosis)
- Secondary diagnoses that are active and affecting management
- Relevant comorbidities — particularly those affecting organ reserve (CKD, COPD, heart failure, diabetes, immunosuppression)
- Baseline functional status before the current illness
3. Summary of ICU Course
The clinical course section in a transfer summary should be more concise than in a discharge summary. The receiving team needs the narrative arc, not every daily detail. Structure it as:
- Admission presentation and initial management (2–3 sentences)
- Key clinical events during the stay (procedures, complications, escalations, de-escalations)
- Current clinical phase — where the patient is in their trajectory (improving, plateauing, deteriorating)
For a 10-day ICU stay, the clinical course in a transfer summary should be 3–5 paragraphs, organised by phase rather than day-by-day.
The clinical course section should answer one central question for the receiving intensivist: what is the clinical story of this patient, and where are we in that story right now? If the receiving doctor can read your summary and brief their team at the bedside without needing additional information, you have written it well.
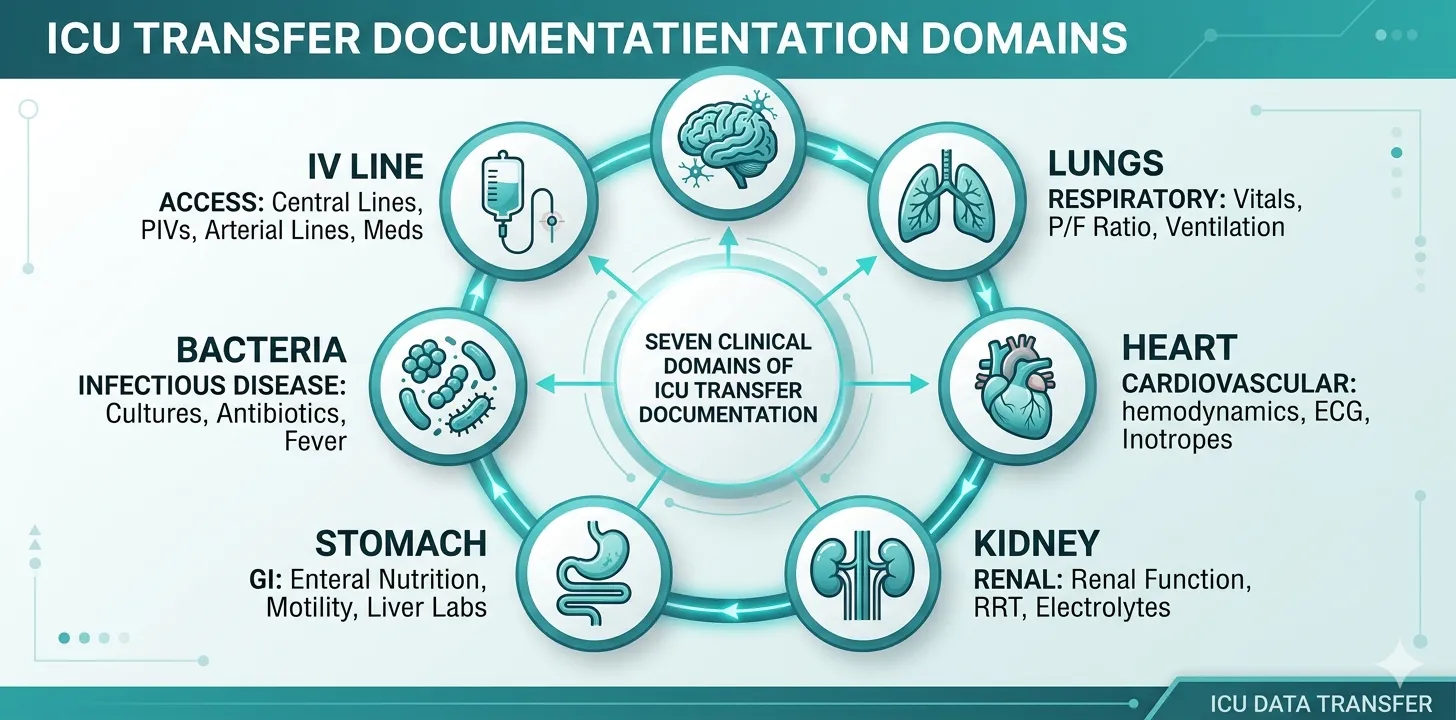
4. Current Clinical Status at Time of Transfer
This is the most critical section of a transfer summary — and the one most frequently underdocumented. It must reflect the patient’s exact clinical state at the time they leave the sending ICU:
Neurological:
- Consciousness level (GCS with component breakdown, or RASS if sedated)
- Pupil reactivity and size
- Any focal neurological deficits
- Sedation and analgesia regimen with current doses
Respiratory:
- Airway status (intubated, tracheostomy, self-ventilating)
- If ventilated: mode, FiO₂, PEEP, tidal volume, respiratory rate, peak pressures
- Most recent blood gas with timestamp
- If self-ventilating: supplemental oxygen device and flow rate, SpO₂
Cardiovascular:
- Heart rate, blood pressure, MAP
- Vasopressor/inotrope infusions with exact doses (µg/kg/min)
- Cardiac rhythm
- Most recent lactate with timestamp
- Fluid balance (cumulative and last 24 hours)
Renal:
- Urine output (last 6 hours and last 24 hours)
- Current creatinine and trend
- If on renal replacement therapy: modality, access, anticoagulation, prescription
- Electrolyte status (K⁺, Na⁺, Ca²⁺, Mg²⁺, PO₄³⁻)
Gastrointestinal and Nutrition:
- Enteral vs parenteral nutrition, current rate and target
- GI issues (ileus, feeding intolerance, GI bleeding)
- Abdominal examination findings if relevant
Infectious Disease:
- Active infections with organisms and sensitivities
- Current antibiotic regimen with day of therapy
- Pending culture results
- Temperature trend
Lines and Drains:
- Every invasive line: type, site, date of insertion
- Drains: type, site, output
- Urinary catheter: date of insertion
A transfer summary that states “patient stable on ventilator support” without specifying the ventilator settings, blood gas values, and vasopressor doses is clinically dangerous. The receiving team cannot safely assume care without knowing the exact parameters. Specificity is not optional — it is the entire point.
5. Procedures Performed During ICU Stay
Document every procedure performed, with:
- Procedure name
- Date
- Indication
- Outcome and any complications
This is particularly important for invasive lines and devices that will transfer with the patient. The receiving team needs to know when a central line was inserted (to assess infection risk and plan removal), when a tracheostomy was performed (to guide weaning strategy), and what surgical interventions have been done.
6. Active Medications at Time of Transfer
This section must list every active medication at the exact time of transfer — not the medications from the morning drug chart or the previous day’s orders:
| Category | What to Document |
|---|---|
| Vasopressors/Inotropes | Agent, concentration, current rate, dose in µg/kg/min |
| Sedation/Analgesia | Agent, current infusion rate, target RASS, last bolus time |
| Antibiotics | Agent, dose, frequency, day of therapy, planned duration |
| Anticoagulation | Agent, dose, indication, last dose time, monitoring parameters |
| Fluids | Maintenance fluids with rate, any blood products ordered |
| Nutrition | Enteral/parenteral, formula, current rate |
| Other | Steroids, insulin infusion, proton pump inhibitors, DVT prophylaxis, eye care |
Document the last dose time for every scheduled medication, especially antibiotics and anticoagulants. Transfer delays are common, and the receiving team needs to know whether the next dose is overdue. A missed antibiotic dose during transfer can set back sepsis management; an overlapping anticoagulant dose can cause bleeding.
Medication documentation scattered across charts and infusion pumps?
Rivara Health captures medications, infusion rates, and dose timings as part of structured daily ICU notes — so your transfer summary has everything in one place.
7. Severity Scores and Trends
Include the most recent severity scores with their component breakdowns:
- SOFA score — with individual organ system scores and the values that generated them
- APACHE II — if calculated at admission
- GCS — with E, V, M component breakdown
- SOFA trend — admission score, peak score, and current score at transfer
Severity scores provide the receiving team with an objective measure of illness severity and trajectory. A patient being transferred with an improving SOFA trend (peak 16, current 10) tells a fundamentally different clinical story than one with a worsening trend (admission 8, current 14).
8. Family Communication and Goals of Care
This section is frequently omitted from transfer summaries — and its absence creates significant problems for the receiving team. Document:
- Current goals of care: Full escalation, ceiling of treatment, limitations (e.g., no CPR, no reintubation), comfort care
- Family understanding of prognosis: What has been communicated and what the family’s expectations are
- Key family contacts: Name, relationship, phone number, and preferred language
- Any advance directives or living wills
- Organ donation discussions if relevant
The receiving team should not have to re-establish goals of care from scratch. If the sending team has had detailed discussions about prognosis and treatment limitations, documenting those discussions in the transfer summary prevents the family from having to relive difficult conversations and ensures continuity of the care plan.
9. Specific Handoff Instructions and Anticipated Problems
This is the section that transforms a transfer summary from a passive record into an active clinical tool. It should include:
- Immediate priorities for the receiving team (e.g., “Plan CT angiography within 6 hours of arrival to assess graft patency”)
- Anticipated clinical problems (e.g., “Patient has failed two extubation attempts — consider tracheostomy if next SBT fails”)
- Medication adjustments expected (e.g., “Vancomycin trough due at 18:00 — adjust dose based on level”)
- Pending results that may change management (e.g., “Tissue biopsy sent — if positive for malignancy, family has requested palliative approach”)
- Triggers for escalation (e.g., “If MAP drops below 65 despite norepinephrine > 0.2 µg/kg/min, consider adding vasopressin”)
Think of the handoff instructions section as your clinical advice to a colleague taking over mid-shift. What would you tell them face-to-face? The things you would say at the bedside — the nuances, the warnings, the plan for the next 24 hours — those belong in writing.
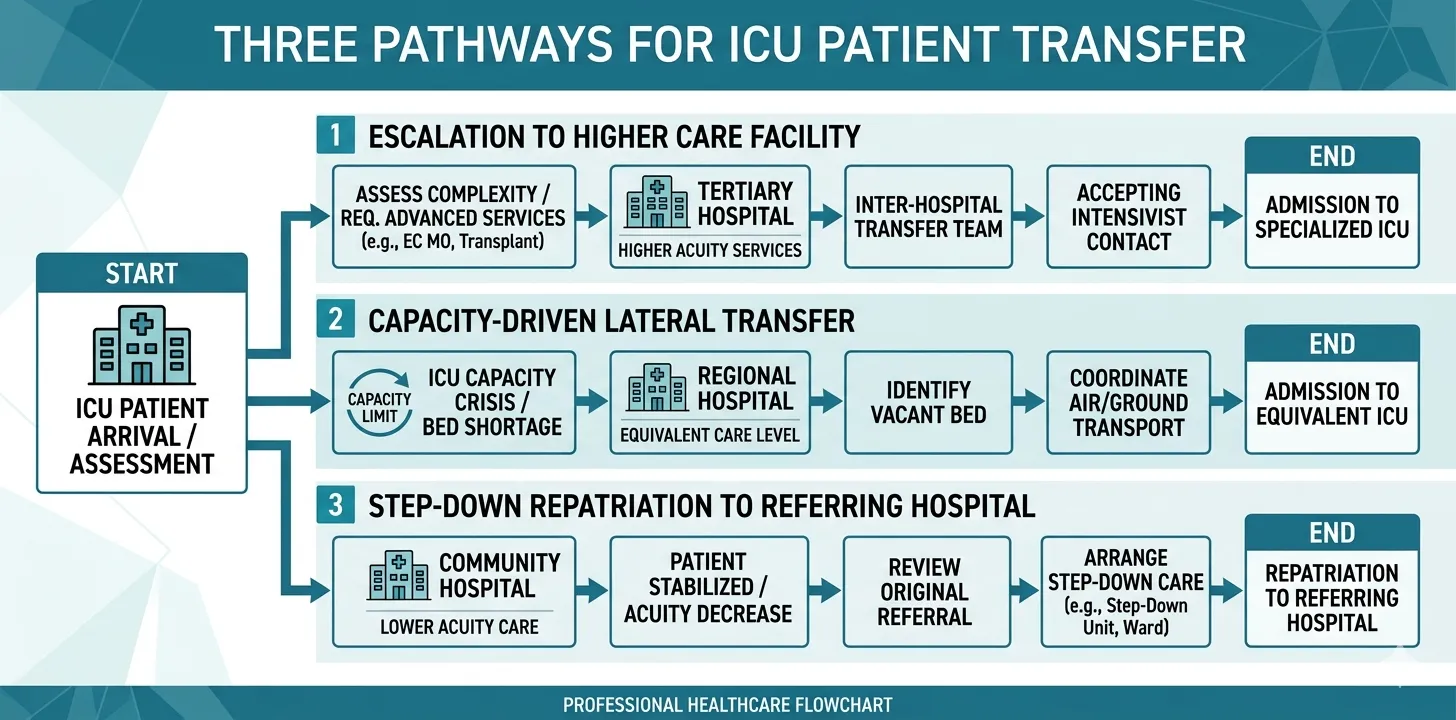
Common Reasons for Inter-Facility ICU Transfers
Understanding why patients are transferred helps structure the documentation. The reason for transfer determines which clinical details require the most emphasis.
Escalation of Care
The most common reason for inter-facility transfer is the need for specialist services or capabilities not available at the sending facility:
- Neurosurgical intervention — aneurysm clipping or coiling, decompressive craniectomy, spinal surgery
- Cardiothoracic surgery — CABG, valve surgery, ECMO initiation
- Interventional radiology — embolisation, TIPS procedure
- Transplant services — organ transplant evaluation or surgery
- Specialist medical care — burns centre, toxicology centre, high-risk obstetric unit
For escalation transfers, emphasise the clinical indication for the specialist service, the current stability for transport, and any interventions performed at the sending facility to temporise the condition.
Capacity Constraints
When ICU bed availability forces transfers, documentation must clearly state that the transfer is driven by capacity rather than clinical need — and must include a detailed assessment of the patient’s transport risk. This has medicolegal significance: a patient who deteriorates during a capacity-driven transfer raises different questions than one transferred for specialist care.
Step-Down or Repatriation
Patients transferred from a tertiary ICU back to a referring hospital for ongoing care require documentation that is oriented toward continued management rather than specialist intervention. Emphasise the ongoing care plan, expected recovery trajectory, and criteria for re-referral.
ICU Transfer Summary vs. Discharge Summary: Key Differences
While an ICU transfer summary and a discharge summary share structural elements, the transfer summary has several distinct requirements:
1. Currency over completeness. A discharge summary can take hours to compile and review because the patient’s care has concluded. A transfer summary must be current — reflecting the patient’s status at the moment of transfer — and is often prepared under time pressure.
2. Active infusion documentation. A discharge summary lists medications the patient goes home on. A transfer summary must list every active infusion with its current rate, concentration, and the time it was last adjusted.
3. Ventilator-specific detail. A discharge summary might note “patient was ventilated for 8 days.” A transfer summary must specify the current ventilator mode, settings, and most recent blood gas — because the receiving team will connect the patient to their ventilator and needs to match the settings.
4. Anticipatory guidance. A discharge summary provides follow-up instructions. A transfer summary provides immediate clinical guidance — what to watch for, what to do next, what to expect in the next 24–48 hours.
5. Real-time communication. Unlike a discharge summary, a transfer summary is typically accompanied by a direct physician-to-physician handoff call. The written summary and the verbal handoff should be consistent and complementary — the summary provides the comprehensive record; the call highlights the most critical elements.
Best Practices for Writing ICU Transfer Summaries
Write Concurrently, Not Retrospectively
Begin drafting the transfer summary as soon as the decision to transfer is made. Update the current clinical status section immediately before the patient leaves. A summary written after the patient has departed is less accurate and less useful.
Use Structured Templates
Free-text transfer summaries are associated with higher rates of information omission. A structured template with mandatory fields for each of the nine components described above ensures completeness even under time pressure.
Include Quantitative Data, Not Qualitative Descriptions
| Instead of… | Write… |
|---|---|
| ”Patient is on moderate ventilator support" | "Volume-control ventilation: TV 420 mL, RR 16, PEEP 10, FiO₂ 0.5, PIP 28" |
| "Blood pressure is low, on vasopressors" | "MAP 62, norepinephrine 0.15 µg/kg/min, vasopressin 0.03 units/min" |
| "Kidneys are not doing well" | "Creatinine 3.8 mg/dL (admission 1.1), UO 15 mL/hr, CRRT initiated Day 4" |
| "Patient is confused" | "GCS 12 (E3V4M5), CAM-ICU positive, on dexmedetomidine 0.4 µg/kg/hr” |
Qualitative descriptions are interpretations; quantitative data is evidence. The receiving team needs the numbers to make their own clinical assessments. Never assume the receiving clinician shares your interpretation of “moderate” or “stable” — provide the data and let them interpret.
Ensure Verbal and Written Handoffs Are Aligned
The physician-to-physician handoff call should follow the same structure as the written summary. Discrepancies between what was said verbally and what was documented create confusion and medicolegal risk. Use the transfer summary as your script for the handoff call.
Document the Transfer Decision Process
Record who made the decision to transfer, why, what alternatives were considered, and whether the patient or family consented. This is particularly important for transfers driven by capacity constraints or when the patient’s clinical condition makes transport risky.
Building transfer summaries from scattered daily notes?
Rivara Health's structured ICU documentation captures every clinical detail during the stay — generating transfer-ready summaries with current medications, ventilator settings, and severity scores.
Medicolegal Considerations for ICU Transfers
Inter-facility transfers carry distinct medicolegal risks that must be addressed through documentation. For a comprehensive overview of medicolegal requirements, see our complete guide to medicolegal documentation in the ICU.
EMTALA and Equivalent Regulations
In the United States, the Emergency Medical Treatment and Labor Act (EMTALA) governs inter-facility transfers. It requires that transfers are medically appropriate, that the sending facility has provided stabilising treatment within its capability, and that the receiving facility has accepted the transfer. Many other jurisdictions have equivalent legislation.
Document:
- Stabilisation measures taken before transfer
- Medical necessity for transfer
- Acceptance by the receiving facility (including the name of the accepting physician)
- Informed consent from the patient or surrogate
Transport Risk Documentation
Critically ill patients face real risks during transport: accidental extubation, loss of IV access, haemodynamic instability, equipment failure. Document the patient’s fitness for transport, the level of medical escort, and the monitoring and equipment accompanying the patient.
Liability Handoff
The medicolegal responsibility for the patient transitions from the sending team to the receiving team at the point of handoff. The transfer summary — combined with the verbal handoff — establishes the moment and content of that transition. Both teams have a shared interest in ensuring the documentation is complete.
In litigation following a poor outcome after inter-facility transfer, both the sending and receiving teams may be scrutinised. The sending team will be asked: “Did you communicate everything the receiving team needed?” The receiving team will be asked: “Did you review the transfer documentation and act on it?” The transfer summary is the evidence for both questions.
ICU Transfer Summary Checklist
Before the patient leaves your ICU, verify that the transfer summary includes:
- Patient identifiers and transfer logistics (sending/receiving facility, accepting physician, transport mode)
- Reason for transfer — specific and documented
- Informed consent for transfer
- Primary and secondary diagnoses at time of transfer
- Concise summary of ICU course
- Current clinical status across all organ systems with quantitative data
- Current ventilator settings and most recent blood gas (with timestamp)
- Current vasopressor/inotrope doses
- All active medications with last dose times
- All invasive lines and drains with insertion dates
- Severity scores (SOFA with components, GCS with breakdown)
- All procedures performed during the stay
- Culture results and current antibiotic regimen with day of therapy
- Family communication, goals of care, and advance directives
- Specific handoff instructions and anticipated problems
- Pending results that may change management
- Direct contact number for the transferring intensivist
For guidance on documentation best practices beyond transfers, see our ICU documentation best practices guide.
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Conclusion
The ICU transfer summary is a specialised document that demands more precision and clinical currency than a standard discharge summary. It is prepared under time pressure, for a patient whose care is ongoing, and for a receiving team that has never seen the patient before. Every section — from the current ventilator settings to the goals-of-care discussions — must be complete, current, and specific.
The principles are consistent regardless of the reason for transfer or the healthcare system: document quantitative data rather than qualitative descriptions; document what is happening right now, not what happened yesterday; and document the clinical plan going forward, including anticipated problems and triggers for escalation.
Inter-facility transfers are high-risk events with significant medicolegal implications. The transfer summary is both the clinical lifeline for the receiving team and the legal evidence that the sending team met the standard of care. Treating it as a checkbox exercise rather than a clinical handoff tool puts the patient — and the treating team — at risk.
Tools like Rivara Health’s ICU documentation platform support this workflow by capturing structured clinical data throughout the ICU stay, ensuring that when a transfer decision is made, the clinical information is already organised and ready to be assembled into a comprehensive transfer summary — rather than scattered across nursing charts, lab systems, and handwritten notes.
Related reading:
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Reduce ICU Documentation Time by 90%
Generate medicolegal-grade ICU discharge summaries in under 2 minutes. Built for Indian hospitals, designed for TPA compliance.