Mechanical ventilation is one of the defining interventions of ICU care, but the goal of ventilation is always eventual liberation from the ventilator. Ventilator weaning accounts for approximately 40% of the total duration of mechanical ventilation in most ICU patients — making it one of the longest and most resource-intensive phases of the ICU stay.
For ICU doctors in India, ventilator weaning decisions carry both clinical and financial consequences. Every additional ventilator day increases the risk of ventilator-associated pneumonia (VAP), ICU-acquired weakness, and other complications. Simultaneously, ventilator days are the single largest driver of ICU billing — and TPA insurance reviewers scrutinise them more closely than any other aspect of the claim.
This guide covers the clinical approach to ventilator weaning, the documentation requirements that satisfy both clinical standards and TPA review, and the common pitfalls that lead to prolonged ventilation and rejected insurance claims.

Understanding the Phases of Mechanical Ventilation
The duration of mechanical ventilation can be divided into three distinct phases, each with different documentation requirements:
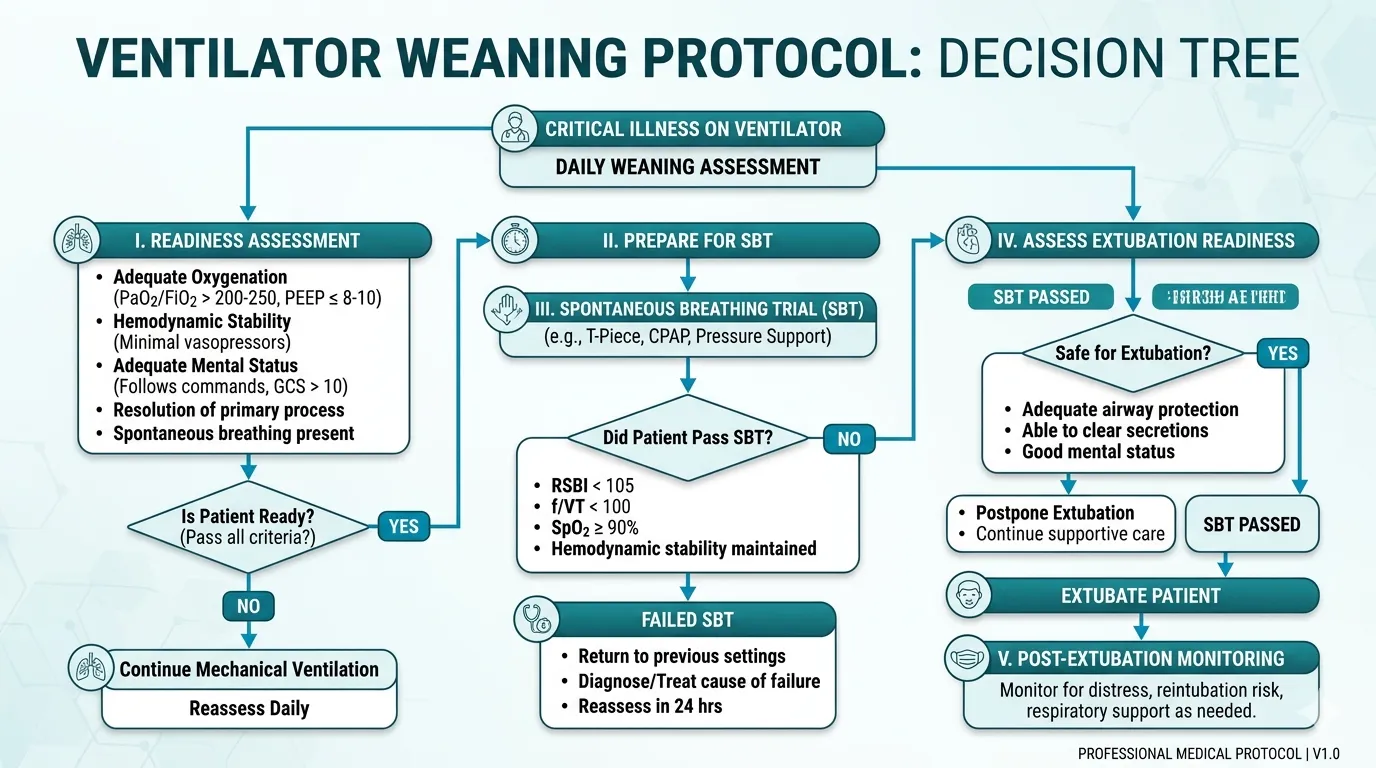
Phase 1: Acute ventilatory support (Days 1–3 typically) The patient is initiated on full ventilatory support — typically assist-control or pressure-controlled ventilation. The underlying cause of respiratory failure is being treated. Documentation during this phase focuses on the indication for ventilation, initial settings, oxygenation (PaO₂/FiO₂ ratio), and the treatment of the underlying condition.
Phase 2: Weaning readiness and trials (variable duration) The underlying condition has improved sufficiently to consider reducing ventilatory support. This phase involves daily assessment of weaning readiness, spontaneous breathing trials (SBTs), and progressive reduction of support. Documentation here is critical for both clinical management and TPA justification.
Phase 3: Extubation and post-extubation monitoring (24–72 hours) The patient has passed a spontaneous breathing trial and is extubated. Monitoring for post-extubation stridor, reintubation need, and respiratory deterioration. Documentation of extubation criteria, timing, and post-extubation course.
TPA reviewers expect to see a clear progression through these three phases. A patient who remains on full ventilatory support at the same settings for 10 days without any weaning attempt documented will be flagged — the reviewer will question whether the ventilation was clinically necessary for the entire duration.
Assessing Weaning Readiness: Daily Screening
Daily assessment of weaning readiness should begin as soon as the patient is stabilised on the ventilator. The following criteria must be met before proceeding to a spontaneous breathing trial:
Objective Weaning Readiness Criteria
| Criterion | Threshold |
|---|---|
| Underlying cause | Resolving or resolved |
| Oxygenation | PaO₂/FiO₂ ≥ 150–200 on FiO₂ ≤ 0.4 and PEEP ≤ 8 cmH₂O |
| Haemodynamic stability | No vasopressors or low-dose vasopressors (norepinephrine ≤ 0.1 µg/kg/min) |
| Neurological status | GCS ≥ 8 (or appropriate for baseline), following commands |
| Adequate cough | Present — assessed clinically |
| Secretion burden | Manageable — not requiring suctioning more than every 2 hours |
| Metabolic status | No severe acidosis (pH ≥ 7.25) or uncorrected electrolyte imbalances |
| Temperature | No significant fever (< 38.5°C) |
These are guideline criteria, not absolute thresholds. Clinical judgment remains essential. A patient with a PaO₂/FiO₂ of 180 on FiO₂ 0.4 may be ready for an SBT despite not meeting the ≥ 200 criterion — if the clinical trajectory is improving and other criteria are met. Document your clinical reasoning when proceeding despite borderline values.
Document the weaning readiness assessment in every daily note — even when the patient does not meet criteria. “Weaning readiness assessment: Not met — patient remains vasopressor-dependent (norepinephrine 0.2 µg/kg/min) and FiO₂ 0.6. Will reassess tomorrow.” This documentation justifies each ventilator day to TPA reviewers.
The Spontaneous Breathing Trial (SBT)
The SBT is the gold standard test for extubation readiness. It involves reducing ventilatory support to a minimal level and observing whether the patient can breathe effectively on their own.
SBT Methods
| Method | Settings | Notes |
|---|---|---|
| T-piece trial | Patient breathes through ETT connected to humidified oxygen (no ventilator support) | Most demanding; tests true unassisted breathing |
| Low PSV | Pressure Support 5–8 cmH₂O + PEEP 5 cmH₂O | Compensates for ETT resistance; most commonly used |
| CPAP | CPAP 5 cmH₂O only | Intermediate difficulty |
SBT Duration
- Standard SBT: 30 minutes to 2 hours
- Recent evidence (ATS/ACCP 2017 guidelines) supports 30-minute trials as sufficient for most patients
- Extended 2-hour trials may be appropriate for patients with prior failed weaning attempts
SBT Success Criteria
The patient passes the SBT if they maintain the following for the full trial duration:
| Parameter | Pass |
|---|---|
| Respiratory rate | < 35/min |
| SpO₂ | ≥ 90% (or baseline for COPD patients) |
| Heart rate | No increase > 20% from baseline |
| Blood pressure | No significant hypertension or hypotension |
| Accessory muscle use | Absent or minimal |
| Agitation or diaphoresis | Absent |
| Rapid shallow breathing index (RSBI) | < 105 breaths/min/L (RR/Vt) |
The Rapid Shallow Breathing Index (RSBI = respiratory rate / tidal volume in litres) is one of the strongest predictors of weaning outcome. An RSBI < 105 predicts successful extubation with approximately 80% accuracy. An RSBI > 105 predicts failure. Calculate and document this for every SBT.
SBT Failure Criteria
Terminate the SBT immediately if any of the following occur:
- Respiratory rate > 35/min sustained for > 5 minutes
- SpO₂ < 88% (or below patient’s baseline)
- Heart rate > 140 or increase > 20% from baseline
- Systolic BP > 180 or < 90 mmHg
- Significant accessory muscle use, paradoxical breathing, or diaphoresis
- Agitation, anxiety, or decreased level of consciousness
When an SBT fails, document specifically why it failed and when the trial was terminated: “SBT (PSV 5/PEEP 5) commenced at 09:00. At 09:22, patient developed respiratory rate 38/min, accessory muscle use, and SpO₂ decline to 87%. SBT terminated at 09:25. Patient returned to prior ventilator settings (PSV 12/PEEP 8, FiO₂ 0.4). Weaning failure attributed to respiratory muscle weakness — will reassess in 24 hours.”
Document every ventilator day — in 3 minutes
Rivara Health's structured daily note captures ventilator mode, parameters, FiO₂, SBT results, and weaning readiness — building the documentation TPA reviewers need.
Extubation: Criteria and Documentation
Pre-Extubation Checklist
Before extubation, verify and document:
- SBT passed (method, duration, parameters maintained)
- Cuff leak test (for patients at risk of post-extubation stridor — prolonged intubation > 7 days, traumatic intubation, large ETT, history of difficult airway)
- Airway patency (adequate cough, manageable secretions)
- Mental status (alert enough to protect airway, follows commands)
- Nil by mouth status (gastric residual volume checked)
- Emergency reintubation equipment at bedside
Post-Extubation Monitoring
Document the following for at least 24–48 hours post-extubation:
- Respiratory rate, SpO₂, and oxygen requirement at 1, 4, 12, and 24 hours
- Presence of stridor, hoarseness, or respiratory distress
- Need for non-invasive ventilation (NIV) or high-flow nasal cannula (HFNC) post-extubation
- Any signs of reintubation necessity
Reintubation within 48 hours of extubation is associated with significantly increased mortality. If reintubation is required, document the indication clearly: “Reintubated at 22:00 for progressive hypoxia (SpO₂ 82% on HFNC 60 L/min FiO₂ 0.6) and worsening respiratory distress with accessory muscle use, 18 hours post-extubation. Likely cause: atelectasis and retained secretions.” Failed extubation is a predictable event — thorough documentation protects the treating team.
Managing Difficult Weaning
Approximately 20–30% of mechanically ventilated patients experience difficult weaning (requiring up to 3 SBT attempts or up to 7 days from the first SBT) or prolonged weaning (> 3 failed SBTs or > 7 days from the first SBT).
Common Causes of Weaning Failure
| Category | Causes |
|---|---|
| Respiratory | Unresolved pneumonia, COPD exacerbation, pleural effusion, diaphragmatic weakness, upper airway oedema |
| Cardiac | Weaning-induced cardiac failure (fluid shifts during SBT increase preload), coronary ischaemia |
| Neurological | ICU-acquired weakness, critical illness polyneuropathy/myopathy, delirium, oversedation |
| Metabolic | Hypothyroidism, malnutrition, electrolyte imbalances (hypophosphataemia, hypomagnesaemia) |
| Psychological | Ventilator dependence, anxiety, panic during SBT |
When a patient fails multiple SBTs, investigate systematically rather than repeatedly attempting the same trial. Check for reversible causes: diaphragmatic ultrasound for weakness, echocardiography for weaning-induced pulmonary oedema (BNP or NT-proBNP before and after SBT), phosphate and magnesium levels, and nutritional status. Document each investigation and its findings.
Tracheostomy in Prolonged Ventilation
If weaning is expected to take more than 10–14 days, tracheostomy should be considered. Document:
- The clinical indication for tracheostomy (prolonged ventilation, failed extubation, airway protection)
- Family counselling and consent
- Timing and method (percutaneous vs surgical)
- Post-tracheostomy course and weaning through the tracheostomy
Tracheostomy is a TPA-scrutinised procedure because it signals prolonged ICU care and carries its own procedural costs. The documentation must establish that tracheostomy was clinically indicated — not performed prematurely or as a convenience. A clear timeline of failed weaning attempts, documented SBT failures, and the rationale for tracheostomy is essential.
Ventilator Documentation for TPA Insurance Claims
Ventilator days are the single most expensive component of ICU billing. TPA reviewers scrutinise ventilator documentation more closely than almost any other element.
What TPA Reviewers Check
- Indication for ventilation: Why was the patient intubated? Was it clinically justified?
- Daily ventilator settings: Are the settings documented for each day? Do they show a progression from full support toward weaning?
- Weaning readiness assessments: Is there evidence of daily screening for readiness to wean?
- SBT documentation: When were SBTs attempted? What were the results? Why did they fail?
- FiO₂ and PEEP progression: Are FiO₂ and PEEP being systematically reduced as the patient improves?
- Extubation timing: Was the patient extubated promptly once weaning criteria were met?
- Reintubation justification: If the patient was reintubated, what was the specific indication?
Documentation Red Flags for TPA
| Red Flag | Why It Triggers Review |
|---|---|
| Same ventilator settings for > 3 days without explanation | Suggests no active weaning management |
| No SBT documented despite criteria being met | Suggests unnecessary prolongation of ventilation |
| FiO₂ 0.4 and PEEP 5 for multiple days without SBT | Patient may be ready for extubation but not being progressed |
| ”Patient on ventilator” without daily parameters | No evidence of active ventilator management |
| Ventilator days inconsistent with severity scores | Low SOFA with prolonged ventilation raises questions |
A TPA reviewer who sees 10 ventilator days billed with only a single note saying “patient on mechanical ventilation” will reject the claim or significantly reduce the approved amount. Each ventilator day must be justified by documented clinical parameters, weaning assessments, and clinical reasoning.
Every ventilator day documented — every day justified
Rivara Health's daily notes capture ventilator mode, parameters, FiO₂, PEEP, SBT results, and weaning readiness — creating the audit trail TPA reviewers require.
Sample Ventilator Documentation for a 10-Day ICU Stay
Here is an example of how ventilator documentation should look in the daily notes:
Day 1: Intubated for acute hypoxic respiratory failure (PaO₂/FiO₂ 120). Settings: PC-AC, PC 16 cmH₂O, PEEP 10, FiO₂ 0.7, RR 18. SOFA respiratory: 3.
Day 3: Oxygenation improving (PaO₂/FiO₂ 190). FiO₂ reduced to 0.5, PEEP reduced to 8 cmH₂O. Remains on vasopressor — not ready for weaning.
Day 5: FiO₂ 0.4, PEEP 6. Vasopressors weaned off. Weaning readiness assessment: Met. Plan SBT tomorrow morning.
Day 6: SBT (PSV 5/PEEP 5) commenced at 08:30. RSBI 78 at 30 minutes. Passed 30-minute SBT with stable parameters (RR 22, SpO₂ 95%, HR 88). Extubated at 09:15. Post-extubation: SpO₂ 94% on 4 L/min O₂ via nasal cannula.
Day 7: Post-extubation Day 1. Stable. SpO₂ 95% on 3 L/min O₂. No stridor. Cough effective.
Day 8: O₂ weaned to 2 L/min. SpO₂ 96%. Tolerating oral feeds.
This documentation tells a clear clinical story: acute respiratory failure requiring full ventilatory support, systematic improvement with FiO₂ and PEEP reduction, daily reassessment of weaning readiness, successful SBT with objective parameters, timely extubation, and stable post-extubation course. A TPA reviewer can approve every ventilator day without question.
Conclusion
Ventilator weaning is both a clinical process and a documentation challenge. The clinical goal — safe, timely liberation from the ventilator — aligns perfectly with the documentation goal: demonstrating to TPA reviewers that each ventilator day was clinically necessary, that weaning was systematically pursued, and that extubation occurred as soon as it was safe.
For ICU doctors, the key principle is straightforward: document the weaning assessment every day. Whether the patient is ready for an SBT or still requires full support, the daily note should reflect a systematic evaluation of weaning readiness with specific clinical parameters.
Tools like Rivara Health’s ICU Summary Generator capture ventilator settings, SOFA scores, and weaning assessments in structured daily notes — ensuring that when the discharge summary is generated, the ventilator documentation meets the standard required for TPA approval.
Related reading: ICU Discharge Summary for TPA Insurance Claims | How AI Is Transforming ICU Discharge Documentation
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Reduce ICU Documentation Time by 90%
Generate medicolegal-grade ICU discharge summaries in under 2 minutes. Built for Indian hospitals, designed for TPA compliance.