Patient handover in the ICU is the highest-risk communication event in hospital medicine. When one clinician transfers responsibility for a critically ill patient to another — at shift change, during transfers between units, or at weekend crossover — every piece of information that fails to transfer becomes a potential adverse event. Studies consistently show that communication failures during handover are the leading root cause of sentinel events in intensive care, contributing to an estimated 80% of serious medical errors that involve miscommunication.
This guide covers the structured frameworks, documentation standards, and practical strategies that reduce handover-related harm — applicable to ICUs worldwide, regardless of size, staffing model, or electronic health record maturity.

Why ICU Handovers Are Uniquely High-Risk
General ward handovers are important. ICU handovers are critical — and the distinction matters.
ICU patients differ from ward patients in ways that make every handover inherently more dangerous:
- Multi-organ involvement. A single ICU patient may have active respiratory failure, haemodynamic instability, acute kidney injury, and delirium simultaneously. Missing any one of these threads during handover can lead to delayed intervention.
- Narrow therapeutic windows. Vasopressor titrations, ventilator weaning trials, and antibiotic timing are measured in hours, not days. A delayed action that would be inconsequential on a ward can be fatal in the ICU.
- High medication complexity. Sedation infusions, paralytic agents, insulin drips, and vasoactive drugs require continuous monitoring. If the incoming clinician does not know the current trajectory, they cannot make safe adjustments.
- Rapid clinical change. An ICU patient’s status can change fundamentally within a single shift. The patient who was stable at 08:00 may be in cardiac arrest by 14:00 — and the quality of the morning handover determines whether warning signs were communicated.
A landmark study in Critical Care Medicine found that ICU patients who experienced a shift change during a clinical deterioration had a 24% higher rate of adverse events compared to patients whose deterioration was managed by a single continuous team. The primary driver was information loss during handover.
The risk is not theoretical. The Joint Commission has identified inadequate handover communication as a contributing factor in over 70% of sentinel events involving ICU patients. Every unstructured handover is a gamble with patient safety.
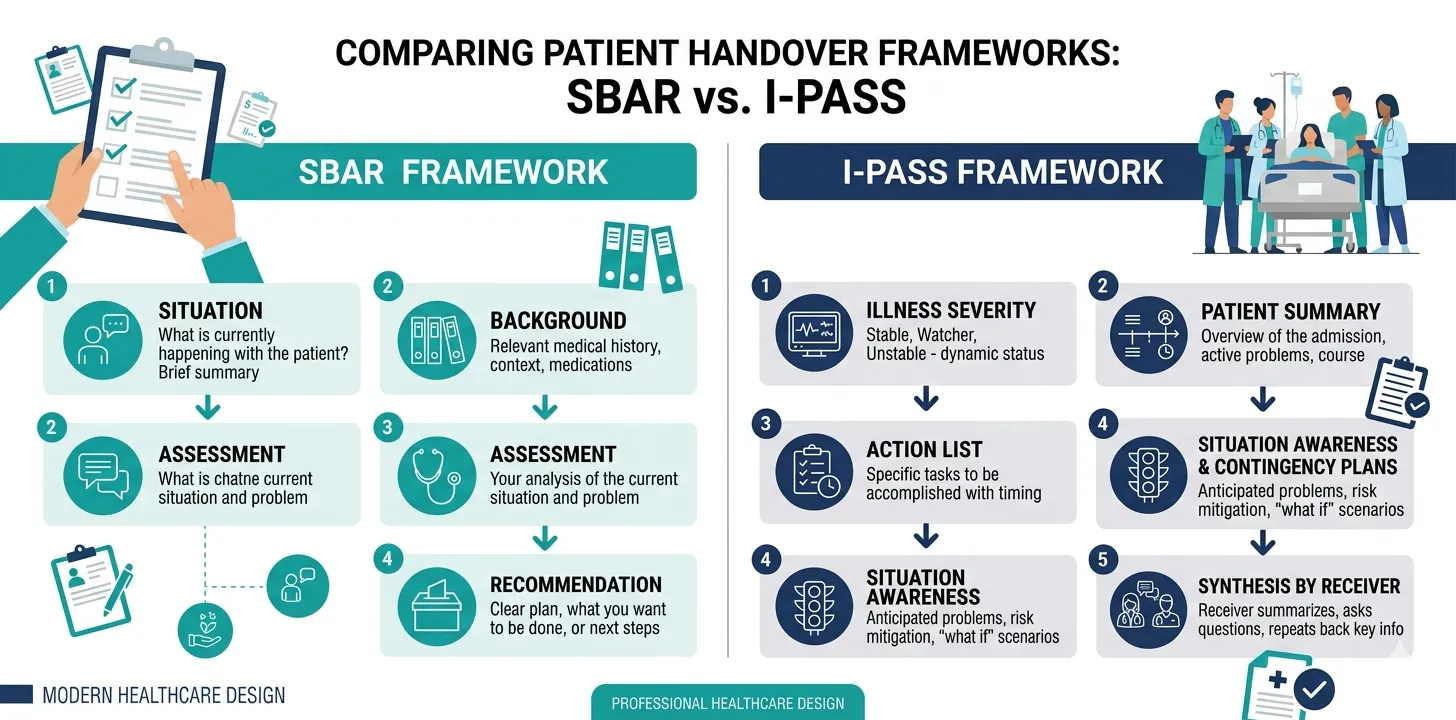
The SBAR Framework
SBAR is the most widely adopted handover communication framework in healthcare. Originally developed by the US Navy for nuclear submarine operations — where miscommunication has catastrophic consequences — it was adapted for clinical use by Kaiser Permanente in the early 2000s and is now endorsed by the WHO, the Joint Commission, and most national patient safety agencies.
SBAR stands for:
S — Situation
State what is happening right now. This is a concise summary of the patient’s current clinical status and the reason for the handover communication.
Example: “Mrs. Patel, bed 4, is a 62-year-old woman, Day 5 of ICU admission for septic shock secondary to urosepsis. She is currently intubated on pressure support ventilation and is being weaned off norepinephrine.”
B — Background
Provide the clinical context that the receiving clinician needs to understand the current situation. This includes the admission diagnosis, relevant comorbidities, key events during the ICU stay, and current treatment plan.
Example: “She was admitted with E. coli bacteraemia from an obstructed ureteric calculus. Percutaneous nephrostomy was placed on Day 2. She required norepinephrine up to 0.25 µg/kg/min in the first 48 hours. Antibiotics were narrowed to ceftriaxone on Day 3 based on sensitivities. Admission SOFA score was 14; today’s SOFA is 6.”
A — Assessment
State your clinical assessment of the patient’s current trajectory. This is where clinical judgement is communicated — not just data, but interpretation.
Example: “She is improving. Vasopressors were weaned to 0.04 µg/kg/min and I expect to stop them within the next 6–8 hours. She passed her SBT this morning and is a candidate for extubation tomorrow if she remains stable.”
R — Recommendation
State what you need the receiving clinician to do. This is the actionable component — specific tasks, monitoring parameters, decision points, and escalation triggers.
Example: “Please wean norepinephrine by 0.02 µg/kg/min every 2 hours if MAP stays above 65. If she becomes hypotensive after stopping, restart at 0.05 and call me. Continue current antibiotics. Repeat lactate at 18:00 — if it is rising, obtain blood cultures and widen antibiotic cover.”
SBAR works because it imposes a cognitive structure on what would otherwise be an unstructured information dump. The receiving clinician knows what to expect at each stage: first the current state, then context, then interpretation, then action items. This predictability reduces cognitive load and information loss.
When using SBAR, lead with what matters most. If the patient is actively deteriorating, the Situation should say so immediately — do not bury the urgency in the Background section. SBAR is a framework, not a straitjacket.
The I-PASS Framework
I-PASS was developed specifically for clinical handovers and has been validated in a large multicentre study published in the New England Journal of Medicine, which demonstrated a 30% reduction in medical errors and a 23% reduction in preventable adverse events following its implementation.
I-PASS stands for:
I — Illness Severity
Categorise the patient’s acuity explicitly: stable, watcher (at risk of deterioration), or unstable (actively deteriorating or requiring urgent intervention). This sets the incoming clinician’s mental model before any details are shared.
P — Patient Summary
A brief synopsis: diagnosis, relevant history, current status. This is the clinical snapshot — equivalent to SBAR’s Situation and Background combined into a concise narrative.
A — Action List
Specific, prioritised tasks that must be completed during the incoming shift. This is the to-do list: pending investigations, medication changes, procedures scheduled, consultations awaited.
S — Situation Awareness and Contingency Planning
What could go wrong, and what should be done if it does. This is the most distinctive element of I-PASS — it forces the outgoing clinician to think prospectively about the patient’s trajectory and communicate contingency plans.
Example: “If her blood pressure drops below MAP 60 after stopping norepinephrine, restart at 0.05 µg/kg/min and repeat a lactate. If lactate is rising, take blood cultures and discuss with microbiology about broadening cover.”
S — Synthesis by Receiver
The receiving clinician summarises what they have understood and asks clarifying questions. This read-back step closes the communication loop and catches misunderstandings before they become clinical errors.
The critical difference between I-PASS and SBAR is the explicit illness severity categorisation and the contingency planning step. SBAR communicates the current state and immediate recommendations. I-PASS additionally forces the outgoing clinician to anticipate what might go wrong — a cognitive step that is often skipped in unstructured handovers but is precisely when the outgoing clinician’s knowledge is most valuable.
Other Handover Frameworks Used in ICU Practice
While SBAR and I-PASS are the most widely studied, several other frameworks address specific handover scenarios:
ISOBAR
Used extensively in Australian and New Zealand ICUs, ISOBAR adds explicit steps for documentation and accountability:
- I — Identification (patient identifiers)
- S — Situation (current clinical status)
- O — Observation (key vital signs, trends, recent changes)
- B — Background (clinical history and context)
- A — Agreed plan (actions required)
- R — Read-back (receiver confirms understanding)
ISOBAR is particularly strong for inter-facility transfers and handovers where the receiving clinician has no prior knowledge of the patient.
SHARED
The SHARED framework emphasises the documentation component of handover — a critical gap in many ICU settings where handovers happen verbally but are never recorded:
- S — Situation
- H — History
- A — Assessment
- R — Risks (what could go wrong)
- E — Expectation (what to watch for)
- D — Documentation (record the handover)
The choice of framework matters less than consistent use of any structured approach. A unit that uses SBAR consistently will outperform one that uses I-PASS inconsistently. Pick a framework, train the team, and audit compliance — the specific framework is secondary to the discipline of using one.
What Must Be Communicated at Every ICU Handover
Regardless of which framework you adopt, certain information must transfer at every ICU shift change. Omitting any of these creates a gap that the incoming clinician may not recognise until it becomes a clinical problem.
1. Current Clinical Status and Trajectory
Not just the numbers — the interpretation. “MAP 68 on norepinephrine 0.08” is data. “MAP trending down over the past 4 hours despite increasing norepinephrine — I am concerned about new septic focus” is clinical communication.
2. Active Problems and Organ Support
A system-by-system summary of active issues:
| System | What to Communicate |
|---|---|
| Respiratory | Ventilator mode, key settings (FiO₂, PEEP), P/F ratio, weaning status, airway concerns |
| Cardiovascular | Haemodynamic status, vasopressor doses and trend, fluid balance, ECG concerns |
| Renal | Urine output trend, creatinine trajectory, RRT status and schedule |
| Neurological | GCS or RASS, sedation plan, delirium status, any focal deficits |
| Infectious | Active infections, current antibiotics, pending culture results, fever status |
| GI/Nutrition | Feeding route and tolerance, bowel function, liver function trends |
| Haematological | Coagulation status, anticoagulation, platelet trends, transfusion needs |
3. Pending Actions and Decisions
Tasks that must be completed during the incoming shift: labs to check, imaging to follow up, consultations awaited, procedures scheduled, family meetings planned.
4. Contingency Plans
What to do if specific things go wrong. This is the most commonly omitted element of handover — and the most valuable. If the outgoing clinician has been managing the patient for 12 hours, they have a mental model of the patient’s trajectory and likely failure modes that the incoming clinician does not yet possess.
5. Goals of Care and Family Communication
Current code status, any limitations of treatment, recent family discussions, and upcoming decision points. In ICU patients where goals of care are evolving, this is as important as any physiological parameter.
Goals of care are one of the most frequently lost pieces of information during handover. A family discussion about transitioning to comfort care that is communicated verbally but not documented — and then lost at shift change — can result in inappropriate escalation, patient suffering, and medicolegal exposure.
Structured daily notes that make every handover easier
Rivara Health captures system-by-system clinical data during the ICU stay — so any clinician can see the patient's full trajectory at a glance, not just the last shift's notes.
Documenting the Handover Itself
A verbal handover that is not documented is, from a medicolegal and quality perspective, a handover that did not happen. Increasingly, accreditation bodies and patient safety organisations require that ICU handovers produce a documented record.
What to Document
The handover record does not need to be lengthy. It should capture:
- Date and time of handover
- Outgoing and incoming clinicians (names and roles)
- Patient list with brief status for each patient
- Key concerns flagged during handover
- Specific action items assigned to the incoming team
- Any disagreements or clarifications discussed
Where to Document
The documentation can take several forms:
- Handover sheet — A printed or digital document updated each shift and passed to the incoming team. Simple but effective.
- EMR-integrated handover — Some electronic health records have handover modules that pull in current patient data and allow free-text annotations. These create a timestamped, auditable record.
- Structured handover tool — Purpose-built tools that combine current clinical data with free-text clinical reasoning and action items.
The best handover documentation combines auto-populated clinical data (current ventilator settings, latest vitals, active infusions) with clinician-entered interpretation and action items. Pure auto-population misses clinical reasoning; pure free-text misses critical data points. The combination is stronger than either alone.
Bedside Handover: The Evidence
There is growing evidence that conducting handover at the bedside — physically in front of the patient — improves safety and communication quality.
A systematic review in Intensive Care Medicine found that bedside handover in the ICU was associated with:
- Fewer omissions of critical clinical information
- Faster identification of clinical changes not captured in documentation
- Improved accuracy of medication and infusion reconciliation
- Increased patient and family engagement in care transitions
The mechanism is straightforward: when you hand over at the bedside, the patient is a visual prompt. The ventilator settings are visible. The infusion pumps are visible. The drain outputs are visible. Discrepancies between what is said and what is physically present are caught in real time.
Bedside handover does not replace structured communication frameworks — it enhances them. Use SBAR or I-PASS at the bedside, not instead of the bedside. The structure ensures completeness; the bedside ensures accuracy.
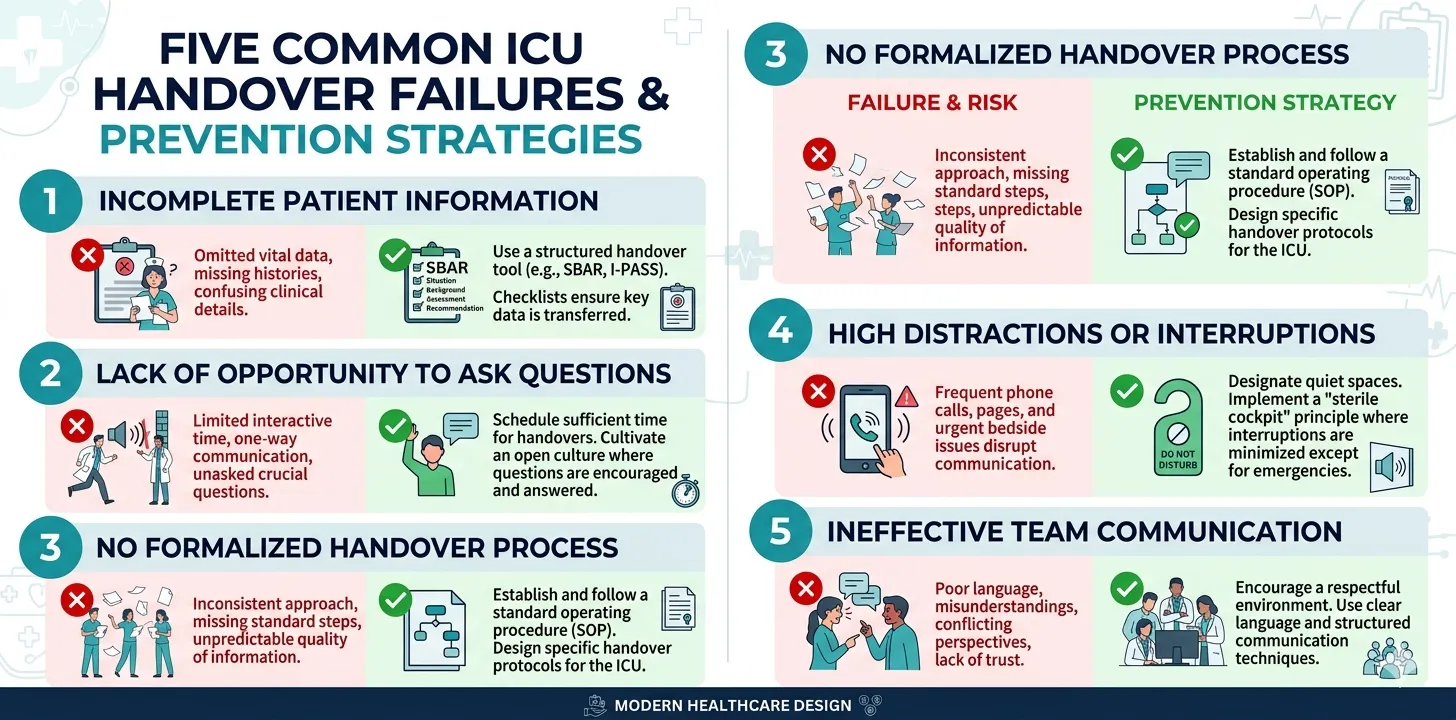
Common Handover Failures and How to Prevent Them
Failure 1: Information Overload Without Prioritisation
Reciting every detail of a complex ICU patient’s 14-day stay at shift change buries the critical information in noise. The incoming clinician cannot absorb it all, and the most important items — the ones that will determine what happens in the next 12 hours — get lost.
Prevention: Lead with illness severity and the one or two things most likely to go wrong. Use the I-PASS severity classification: is this patient stable, a watcher, or unstable? This frames everything that follows.
Failure 2: No Contingency Planning
The outgoing clinician knows the patient’s trajectory intimately. They have spent hours at the bedside and have a nuanced mental model of likely failure modes. If they leave without communicating this — “if X happens, do Y” — the incoming clinician must rebuild that mental model from scratch, often too late.
Prevention: Make contingency planning a mandatory component of every handover. I-PASS builds this in explicitly. If using SBAR, add it to the Recommendation step.
Failure 3: One-Way Communication
Handover that consists of the outgoing clinician talking and the incoming clinician listening is not communication — it is a monologue. Without questions, clarification, and synthesis by the receiver, misunderstandings go undetected.
Prevention: Build in a receiver synthesis step. After the handover, the incoming clinician summarises the key points and action items. This read-back catches errors before they reach the patient.
Failure 4: Interruptions and Distractions
ICU handovers conducted in noisy corridors, interrupted by phone calls, or rushed between emergencies are inherently unsafe. Every interruption increases the risk of information loss.
Prevention: Designate a protected handover time and space. Some ICUs implement a “sterile cockpit” rule — borrowed from aviation — where non-emergency interruptions are prohibited during handover. The evidence supports this: units that implemented protected handover time saw a 40% reduction in handover-related errors.
Failure 5: Failure to Hand Over Goals of Care
Clinical parameters transfer well in structured handovers. What often does not transfer is the human context: family dynamics, goals-of-care discussions, emotional state of the family, and the nuances of shared decision-making. A patient who is transitioning toward comfort care requires a completely different management approach than one who is being aggressively treated — and this context must transfer at every shift change.
Prevention: Include a dedicated goals-of-care section in every handover, not as an afterthought but as a core component.
Measuring Handover Quality
Implementing a handover framework is only the first step. Sustaining it requires measurement. Key metrics to track include:
| Metric | How to Measure | Target |
|---|---|---|
| Framework compliance | Audit: percentage of handovers using the structured framework | > 90% |
| Information completeness | Checklist audit: are all required elements communicated? | > 95% for critical elements |
| Receiver satisfaction | Post-handover survey: did the incoming clinician feel adequately informed? | > 85% satisfaction |
| Handover-related adverse events | Incident reports flagging handover as a contributing factor | Trending downward |
| Handover duration | Time from start to finish | 2–3 minutes per patient (not a speed metric — too short suggests incompleteness) |
Auditing handover quality is one of the highest-yield patient safety interventions available to an ICU. It costs nothing, requires minimal infrastructure, and directly addresses the leading cause of sentinel events. Yet most ICUs audit clinical outcomes without ever auditing the communication process that drives them.
Linking Handover Documentation to Discharge Summaries
Handover documentation and discharge documentation are not separate activities — they are the same clinical narrative at different time scales. Daily shift handovers capture the micro-level: what happened in the last 12 hours, what needs to happen in the next 12. The discharge summary captures the macro-level: the full arc of the ICU stay from admission to discharge.
When daily handover notes are structured and documented, they become the raw material for the discharge summary. A well-documented series of shift handovers — each capturing the key events, decisions, and clinical reasoning for that period — makes writing the discharge summary dramatically easier because the information already exists in an organised form.
This is the approach that tools like Rivara Health’s ICU Summary Generator take: structured daily documentation that serves both immediate handover needs and downstream summary generation. The daily notes capture severity scores, medication changes, procedures, and clinical assessments in a structured format — and at discharge, the AI synthesises them into a complete, coherent summary.
The documentation you do at every shift change is not wasted effort — it is the foundation of every downstream document.
Daily notes that power both handovers and discharge summaries
Rivara Health turns structured shift-by-shift documentation into complete ICU discharge summaries — automatically, in under 2 minutes.
Building a Handover Culture in Your ICU
Frameworks and checklists are necessary but not sufficient. Sustainable handover improvement requires a culture change — one where structured communication is expected, valued, and reinforced.
Start with leadership. Consultants and senior intensivists who model structured handover set the norm. If the most experienced clinician in the unit uses SBAR, trainees will follow.
Train explicitly. Do not assume that clinicians know how to hand over effectively. Simulation-based handover training — where clinicians practise handovers with standardised patients and receive feedback — has been shown to improve both communication quality and clinical outcomes.
Audit and feed back. Measure compliance with the chosen framework, share results with the team, and celebrate improvement. Audit data that stays in a quality office filing cabinet changes nothing. Data shared with the frontline team at monthly meetings drives improvement.
Make it easy. If the handover framework requires 15 minutes per patient, it will not survive contact with a busy 20-bed ICU. The framework must be efficient enough to use consistently — 2–3 minutes per patient is the target — while still capturing the essential elements.
Standardise the format, not the content. Every patient is different. The framework provides the structure; the clinician provides the clinical judgement. Do not let the framework become a rigid checklist that strips away the nuanced clinical reasoning that makes handovers valuable.
For more on building sustainable ICU documentation practices, including how structured daily notes support both handover and discharge workflows, see our documentation best practices guide.
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Conclusion
ICU patient handover is the most frequent high-risk communication event in critical care medicine. Every shift change, every patient transfer, every weekend crossover is an opportunity for information to be lost — and for that loss to cause patient harm.
Structured frameworks like SBAR, I-PASS, ISOBAR, and SHARED provide the scaffolding for safe communication. But frameworks alone are not enough. Effective handover requires documentation, bedside verification, contingency planning, receiver synthesis, and a unit culture that treats communication with the same rigour as clinical procedures.
The evidence is clear: structured handover reduces adverse events, improves information transfer, and protects both patients and clinicians. The investment required is minimal — training, a chosen framework, protected handover time, and a commitment to audit and improve.
For ICU teams looking to strengthen their documentation practices beyond handover — from daily progress notes through to complete discharge summaries and severity scoring — tools like Rivara Health’s ICU Summary Generator connect the dots between shift-level documentation and the final clinical record.
The safest handover is one where no critical information is lost. The best way to ensure that is to document it — structured, standardised, and every single time.
Related reading:
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Reduce ICU Documentation Time by 90%
Generate medicolegal-grade ICU discharge summaries in under 2 minutes. Built for Indian hospitals, designed for TPA compliance.