Discharge summaries are the final clinical deliverable of an ICU admission. They consolidate days or weeks of complex care into a single document used for handover, insurance claims, medicolegal protection, and continuity of care. Every ICU doctor writes them. Few enjoy the process.
The emergence of AI-powered documentation tools has introduced a genuine alternative to the manual workflow that most hospitals still rely on. But the question is not simply “Is AI faster?” — it is whether AI-generated discharge summaries are accurate enough, consistent enough, and legally defensible enough to replace or augment the traditional process.
This article compares manual and AI-generated ICU discharge summaries across the dimensions that matter most to clinical teams: accuracy, speed, consistency, medicolegal defensibility, and cost. The goal is a balanced assessment — not a sales pitch.
Why Discharge Summaries Matter More Than Most Documentation
Before comparing methods, it is worth grounding why discharge summaries carry disproportionate weight relative to other clinical documents.
A discharge summary is the single document that travels with the patient after the ICU stay ends. It is read by the receiving ward team, the outpatient follow-up physician, the insurance reviewer, and — in the event of a dispute — the court. It must simultaneously serve as:
- A clinical handover tool — communicating the patient’s ICU course, unresolved problems, and follow-up plan
- An insurance document — justifying the level of care, procedures performed, and length of stay
- A medicolegal record — serving as contemporaneous evidence of clinical decision-making
- An administrative record — supporting hospital audits, quality metrics, and accreditation requirements
No other single document in the patient’s chart serves all four purposes. This is why accuracy and completeness are non-negotiable — and why the method of production matters.
For a deeper look at what goes into a well-structured summary, see our complete guide to ICU discharge summaries.
The discharge summary is not just a summary. It is the definitive narrative of the ICU stay — the version that outlasts the treating team’s memory, the bedside notes, and often the patient’s own recollection. Getting it right is a clinical responsibility, not a clerical one.
The Manual Process: How Most ICU Teams Work Today
In the majority of hospitals worldwide, the discharge summary is written manually by the treating physician or a junior doctor under supervision. The typical workflow looks like this:
- The patient is discharged or transferred from the ICU
- The doctor gathers bedside notes, nursing charts, lab printouts, and procedure records
- The doctor reconstructs the clinical narrative from these fragmented sources — often from memory for events not adequately documented
- The summary is typed into a hospital information system, a word processor, or (in many settings) handwritten
- The document is reviewed, signed, and filed
This process has been the standard for decades. It works — in the sense that summaries get produced. But it has well-documented limitations.
Strengths of Manual Summaries
Clinical nuance. An experienced physician can capture subtlety that no algorithm currently replicates. The reasoning behind a decision to withhold dialysis despite rising creatinine, the family dynamics that influenced a goals-of-care conversation, the clinical gestalt that led to an early escalation — these are the kinds of judgment calls that manual documentation captures well.
Contextual awareness. The treating doctor understands which details are clinically significant for the specific patient. They can emphasise the important and omit the trivial in ways that reflect genuine clinical understanding.
Adaptability. Manual summaries can be tailored to the audience. A summary intended for a tertiary referral centre can differ in emphasis from one going to a primary care physician — and the doctor can make that judgment in real time.
No technology dependency. The process requires nothing more than the clinical record and a writing tool. There is no software to learn, no data pipeline to maintain, no risk of system downtime.
Limitations of Manual Summaries
Time. This is the most widely cited problem. A comprehensive summary for a 10–15 day ICU stay takes 2–3 hours to write manually. For complex patients with multi-organ failure, ventilator management, and multiple procedures, it can take longer. This time is typically drawn from the doctor’s post-shift hours or from time that could be spent on active patient care.
Incomplete recall. When summaries are written at discharge, the doctor must reconstruct events that occurred days or weeks earlier. Memory degrades. Details are omitted — not because they are unimportant, but because they are forgotten.
Inconsistency. Without a structured template, the content and quality of summaries vary widely between doctors, between shifts, and between hospitals. What one physician includes in exhaustive detail, another may omit entirely.
Delayed completion. In high-volume ICUs, summaries are often completed days after discharge. This introduces additional recall errors and delays insurance claim processing.
Omission of objective data. Manual summaries frequently lack specific lab values, exact vasopressor doses, daily SOFA scores, and precise timestamps — the very data points that insurance reviewers and courts scrutinise most closely.
Studies consistently show that manually written discharge summaries have significant omission rates. Research published in the Journal of Hospital Medicine found that up to 40% of manual summaries were missing at least one clinically important element — including pending test results, medication changes, and follow-up plans. These omissions are not minor: they directly impact patient safety and downstream care.
The AI-Assisted Process: How It Works
AI-generated discharge summaries use large language models (LLMs) to synthesise structured clinical data into a coherent narrative document. The critical distinction is that the AI does not replace the clinician’s documentation — it transforms structured data that was collected during the stay into a formatted output.
The typical AI-assisted workflow:
- During the ICU stay, clinicians enter structured daily notes — vitals, medications, procedures, lab values, clinical assessments
- At discharge, the system aggregates this structured data into a complete clinical timeline
- The AI model generates a narrative discharge summary from the structured dataset
- The physician reviews, edits if necessary, and approves the final document
This is the approach used by tools like Rivara Health’s ICU Summary Generator, which collects structured data throughout the stay and uses Google Gemini to produce the final summary.
Strengths of AI-Generated Summaries
Speed. An AI system can generate a comprehensive discharge summary in under 2 minutes — compared to 2–3 hours manually. This is the most immediately tangible benefit.
Completeness. Because the AI works from structured data, it does not forget. Every daily note, every lab value, every procedure logged during the stay is included in the synthesis. There are no gaps caused by recall failure.
Consistency. AI-generated summaries follow a consistent structure every time. The format, headings, level of detail, and inclusion criteria do not vary by physician, time of day, or workload pressure.
Objective data inclusion. Daily SOFA scores, exact vasopressor doses, specific lab values with timestamps — the AI includes these automatically because they exist in the structured dataset. These are precisely the data points most commonly missing from manual summaries.
Timeliness. Summaries can be generated immediately at discharge, eliminating the backlog that plagues busy ICUs.
Limitations of AI-Generated Summaries
Dependent on input quality. The AI summary is only as good as the data entered during the stay. If daily notes are incomplete, rushed, or inconsistent, the generated summary will reflect those gaps. The principle is simple: garbage in, garbage out.
Limited clinical reasoning. Current AI models can synthesise data into narrative, but they cannot replicate the clinical reasoning that experienced physicians bring. The AI will not explain why a decision was made — only what was done. If the rationale is not documented in the daily notes, it will not appear in the summary.
Risk of plausible-sounding errors. Large language models can occasionally generate text that sounds clinically plausible but is factually incorrect — a phenomenon often called “hallucination.” While structured data inputs significantly reduce this risk compared to free-text AI generation, physician review remains essential.
Technology dependency. AI-assisted workflows require reliable internet access, a functioning software platform, and clinician familiarity with the tool. In settings with unreliable infrastructure or resistance to digital workflows, this is a genuine barrier.
Not a replacement for clinical judgment. The AI does not decide what is clinically significant — it processes what was documented. A physician still needs to review the output and ensure that the narrative accurately reflects the clinical reality.
The key distinction is between AI as author and AI as synthesiser. Current tools synthesise structured data into narrative form — they do not independently author clinical assessments. The physician remains the clinical authority; the AI handles the labour-intensive transformation of data into document.
Head-to-Head Comparison
The following table compares manual and AI-generated discharge summaries across the dimensions most relevant to ICU teams.
| Dimension | Manual Summaries | AI-Generated Summaries |
|---|---|---|
| Time to produce | 2–3 hours per complex patient | Under 2 minutes |
| Completeness | Variable; recall-dependent | High; draws from all structured entries |
| Consistency | Varies by physician and workload | Uniform structure every time |
| Clinical nuance | High — captures reasoning and judgment | Limited to what was documented in notes |
| Objective data | Often incomplete (SOFA, exact doses) | Automatically included from structured data |
| Timeliness | Often delayed by hours or days | Available immediately at discharge |
| Error profile | Omission errors (forgetting details) | Commission errors (possible hallucination) |
| Technology requirement | None | Requires software platform and internet |
| Cost | Physician time (high opportunity cost) | Software cost (typically lower) |
| Physician review needed | Self-authored (inherent review) | Mandatory review before approval |
Neither approach is categorically superior. Manual summaries excel at capturing clinical reasoning and nuance. AI summaries excel at completeness, consistency, and speed. The strongest documentation workflows combine both — using AI to generate the comprehensive draft and physician review to ensure clinical accuracy.
What if the first draft wrote itself?
Rivara Health generates complete ICU discharge summaries from your structured daily notes — ready for physician review in under 2 minutes.
Accuracy: The Central Question
When clinicians evaluate AI documentation tools, accuracy is the first and often the only question: Is the AI output correct?
The answer is nuanced. Accuracy in discharge summaries has two components:
Factual accuracy — Are the stated lab values, medication doses, procedures, and timelines correct? For AI summaries generated from structured data, factual accuracy is generally high because the system is referencing documented values, not generating them from nothing. The risk of factual error is proportional to the quality of the input data.
Narrative accuracy — Does the summary tell the right clinical story? Does it correctly represent the trajectory of illness, the response to treatment, and the reasoning behind clinical decisions? This is where manual summaries have an advantage — and where AI summaries require careful physician review.
The error profiles are fundamentally different. Manual summaries suffer from omission errors — things that should have been included but were forgotten. AI summaries are more susceptible to commission errors — statements that are included but may not accurately reflect clinical intent. Understanding this distinction is essential for designing effective review workflows.
Medicolegal Defensibility
In medicolegal proceedings, the discharge summary is often the primary document reviewed. Its defensibility depends on three factors:
- Completeness — Were all significant events, decisions, and outcomes documented?
- Contemporaneity — Was the documentation created at or near the time of the events described?
- Traceability — Can each claim in the summary be traced to a source record?
| Legal Factor | Manual | AI-Generated |
|---|---|---|
| Completeness | Often incomplete at discharge | Comprehensive if daily notes are complete |
| Contemporaneity | Written after discharge (delayed) | Generated from daily entries (near real-time data) |
| Traceability | Difficult — memory-based reconstruction | Strong — linked to timestamped structured data |
| Audit trail | Limited | Full trail of entries with timestamps |
| Physician accountability | Author is the physician | Physician reviews and approves AI output |
For a comprehensive discussion of medicolegal documentation requirements in critical care, see our guide on AI in critical care documentation.
In legal proceedings, a summary that is comprehensive and traceable to source data is more defensible than one that relies on the physician’s memory weeks after the events. This is true regardless of whether the summary was written manually or generated by AI — what matters is the evidentiary chain from clinical event to documented record.
Insurance and TPA Considerations
Insurance reviewers evaluate discharge summaries against specific criteria. They look for documented justification of ICU admission, evidence of illness severity (typically SOFA or APACHE scores), procedure documentation with clinical indication, and a clear clinical course narrative.
Manual summaries frequently trigger claim rejections or queries because of:
- Missing severity scores or scores without supporting lab values
- Vague procedure documentation (“central line placed” without indication, site, or date)
- Gaps in the daily clinical course narrative
- Missing medication details (especially vasopressor doses)
AI-generated summaries from structured data address these pain points directly — the severity scores are calculated automatically, procedures are logged with timestamps and details, and the daily course is synthesised from actual entries rather than reconstructed from memory.
However, AI summaries can create their own issues with insurance reviewers:
- Overly uniform language across patients may prompt reviewers to suspect template-based or copy-paste documentation
- AI-generated text that does not match the physician’s documented notes elsewhere in the chart can raise consistency questions
- Some reviewers may not yet be familiar with AI-generated documentation and may scrutinise it more closely
Regardless of the generation method, the discharge summary must align with the rest of the clinical record. An AI-generated summary that includes SOFA scores not reflected in the nursing charts or daily progress notes will raise more questions than it answers. Consistent documentation across all record types is essential.
Cost Analysis: Physician Time vs Software Investment
The cost comparison is often framed as “free vs paid,” but this misrepresents the economics.
Manual documentation is not free. A senior ICU physician spending 2–3 hours on a discharge summary represents a significant opportunity cost — time that could be spent on direct patient care, teaching, or clinical decision-making. In high-volume ICUs managing 5–10 discharges per week, this translates to 10–30 hours of physician time consumed by documentation alone.
AI tools have a direct cost — either per-use fees, subscription costs, or institutional licensing. But when measured against the physician time they replace, the return on investment is typically substantial.
| Cost Factor | Manual | AI-Assisted |
|---|---|---|
| Physician time per summary | 2–3 hours | 10–15 minutes (review and approval) |
| Software cost | None | Varies by platform |
| Delayed discharge cost | Potential bed-day charges from documentation delays | Reduced — summary available immediately |
| Claim rejection cost | Higher due to documentation gaps | Lower with structured, complete summaries |
| Training cost | Minimal (existing skill) | Initial onboarding required |
For strategies to reduce documentation burden without sacrificing quality, see our guide on reducing ICU documentation time.
When Manual Is Still the Right Choice
AI is not the right tool for every situation. Manual documentation remains preferable — or necessary — in several scenarios:
Highly complex clinical reasoning. When the clinical course involves difficult judgment calls — withdrawing life-sustaining treatment, navigating conflicting specialist opinions, managing rare presentations — the physician’s narrative voice carries weight that AI synthesis cannot replicate.
Incomplete digital data. In hospitals where daily notes are not entered in structured digital format, there is no dataset for the AI to synthesise. The manual approach remains the only option until upstream data collection is digitised.
Low-volume ICUs. For units with very few discharges per week, the time investment in learning and maintaining an AI tool may not justify the time savings. The break-even point depends on unit volume and physician availability.
Regulatory or institutional constraints. Some hospitals or jurisdictions may not yet have policies governing AI-generated clinical documents. Until regulatory frameworks catch up, some institutions may require manually authored summaries.
The decision between manual and AI-assisted documentation is not binary. Many ICU teams adopt a hybrid model: AI generates the comprehensive first draft from structured data, and the physician reviews, annotates clinical reasoning, and approves the final version. This captures the efficiency of AI and the judgment of the clinician.
When AI Makes the Bigger Difference
AI-assisted documentation delivers its greatest value in specific contexts:
High-volume ICUs. When a team is managing multiple discharges per day, the cumulative time savings are transformative. Documentation that would consume an entire shift can be reduced to an hour of review.
Long ICU stays. For patients with stays exceeding 10–14 days, the amount of clinical data to synthesise is enormous. AI handles volume effortlessly — the summary for a 30-day stay takes the same 2 minutes as a 3-day stay.
Insurance-heavy environments. In healthcare systems where insurance claim processing depends heavily on documentation quality, the structured completeness of AI-generated summaries directly reduces rejection rates.
Medicolegal risk mitigation. The combination of timestamped structured data, automated severity scoring, and consistent documentation creates a stronger evidentiary record than memory-based manual summaries.
Standardisation across teams. In large ICUs with rotating staff, AI ensures every discharge summary meets the same quality standard regardless of which physician is on duty.
See the difference structured documentation makes
Rivara Health's ICU Summary Generator produces complete, insurance-ready discharge summaries from your daily clinical notes. Free to use — no installation required.
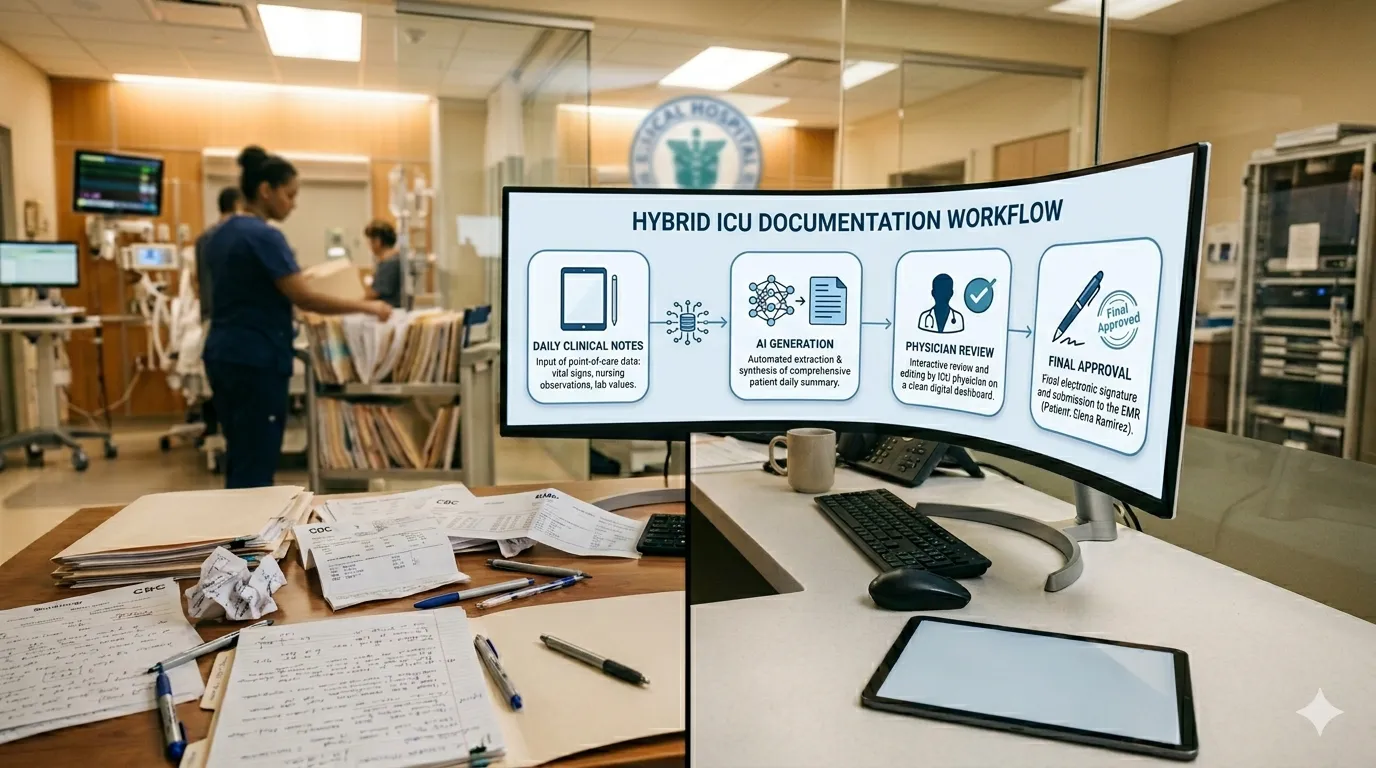
Building the Optimal Workflow
The strongest ICU documentation workflows are not purely manual or purely AI — they are intentionally designed to leverage the strengths of both.
Step 1: Structured daily documentation. Clinicians enter structured daily notes during the ICU stay — vitals, medications, procedures, lab values, clinical assessments. This takes 3–5 minutes per day as part of the existing ward round. This is the foundation that makes everything else possible.
Step 2: AI-generated first draft. At discharge, the AI synthesises the complete dataset into a narrative discharge summary. This draft is comprehensive, consistently formatted, and includes all objective data points.
Step 3: Physician review and annotation. The physician reviews the AI draft, corrects any inaccuracies, adds clinical reasoning that was not captured in the structured notes, and adjusts emphasis as needed. This review typically takes 10–15 minutes.
Step 4: Approval and export. The final document is approved, signed, and exported for distribution to the receiving team, insurance, and hospital records.
This workflow preserves physician oversight while eliminating the 2–3 hours of reconstruction that the manual process demands. The doctor’s time is spent on review and judgment rather than recall and typing.
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Conclusion
The comparison between manual and AI-generated discharge summaries is not a contest with a single winner. Each approach has genuine strengths and real limitations.
Manual summaries capture clinical reasoning, nuance, and physician judgment in ways that current AI cannot replicate. They require no technology infrastructure and are familiar to every clinician.
AI-generated summaries deliver speed, completeness, consistency, and structured data inclusion that manual processes struggle to match — especially at scale. They are particularly valuable for long ICU stays, high-volume units, and insurance-heavy workflows.
The most effective approach for most ICU teams is a hybrid workflow: AI generates a comprehensive, structured first draft from daily clinical data, and the physician reviews, annotates, and approves the final document. This combination delivers the efficiency of automation with the clinical authority of physician oversight.
What matters most is not the method of production — it is the quality of the final document. A discharge summary that is complete, accurate, timely, consistent, and traceable to source data serves the patient, the treating team, the insurer, and the legal record. Whether that document was written by hand or generated by AI is secondary to whether it meets those standards.
Further reading: Complete Guide to ICU Discharge Summaries · AI in Critical Care Documentation · How to Reduce ICU Documentation Time
Medical Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. Rivara Health provides documentation tools — clinical judgement remains with the treating physician.
Reduce ICU Documentation Time by 90%
Generate medicolegal-grade ICU discharge summaries in under 2 minutes. Built for Indian hospitals, designed for TPA compliance.